Download as PDF, PPTX
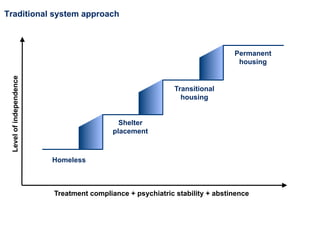
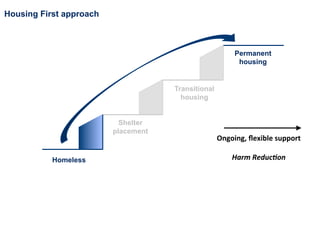
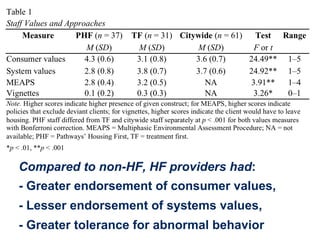
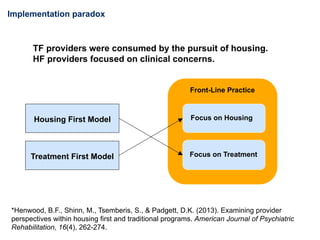
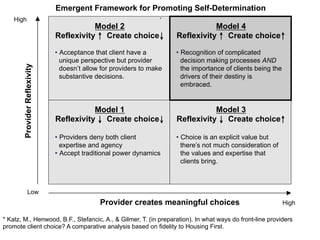
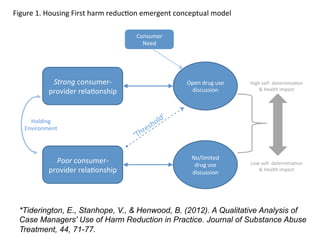

The document discusses the distinctions in frontline practices between Housing First (HF) programs and traditional approaches to homelessness. It emphasizes the unique service delivery, recovery-oriented models, and harm reduction frameworks employed by HF providers that focus on client choice and support. The conclusion highlights the need for practical applications of harm reduction and considerations for varying provider languages and strategies across different demographics.

































































































