Downloaded 11 times
![Intensive Service Interventions for People with Disabilities: Helping Families Stabilize & Thrive 2011 National Conference on Ending Family Homelessness Devra Edelman Director of Programs Hamilton Family Center February 11, 2011 [email_address]](https://image.slidesharecdn.com/6-7devraedelman-110301122538-phpapp02/85/6-7-Intensive-Service-Interventions-for-People-with-Disabilities-1-320.jpg)
![Intensive Service Interventions for People with Disabilities: Helping Families Stabilize & Thrive 2011 National Conference on Ending Family Homelessness Devra Edelman Director of Programs Hamilton Family Center February 11, 2011 [email_address]](https://image.slidesharecdn.com/6-7devraedelman-110301122538-phpapp02/75/6-7-Intensive-Service-Interventions-for-People-with-Disabilities-1-2048.jpg)

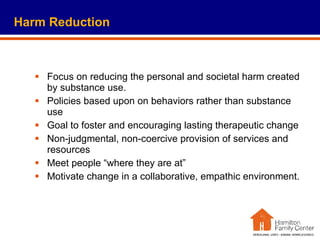
![Program staff feel more confident working with clients How would you rate your skills dealing with [children/ parents] with mental health problems? Highly skilled Not skilled at all Before consultant After consultant Before consultant After consultant Both changes represent statistically significant gains](https://image.slidesharecdn.com/6-7devraedelman-110301122538-phpapp02/85/6-7-Intensive-Service-Interventions-for-People-with-Disabilities-16-320.jpg)
![Contact: Devra M. Edelman Director of Programs Hamilton Family Center 415-409-2100 x122 [email_address] www.hamiltonfamilycenter.org](https://image.slidesharecdn.com/6-7devraedelman-110301122538-phpapp02/85/6-7-Intensive-Service-Interventions-for-People-with-Disabilities-20-320.jpg)

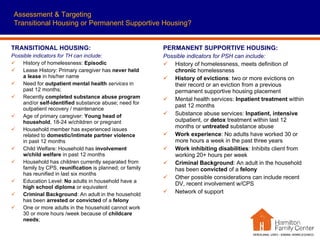
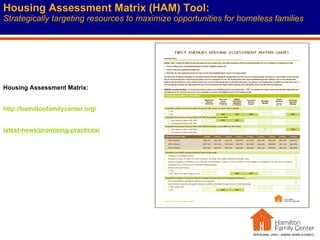
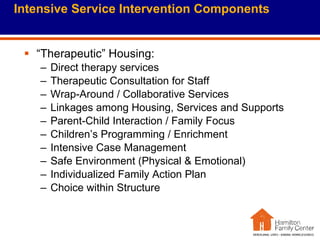
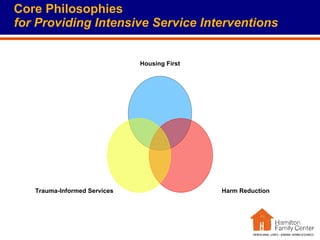
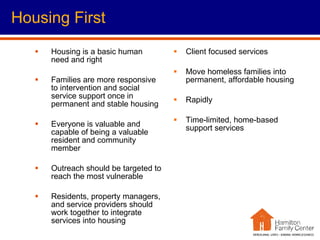
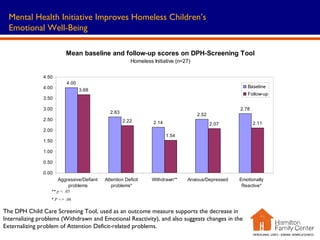
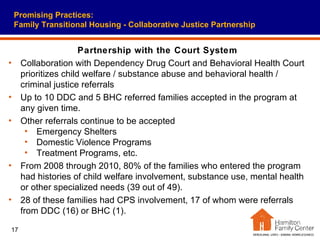
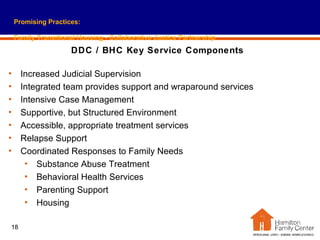
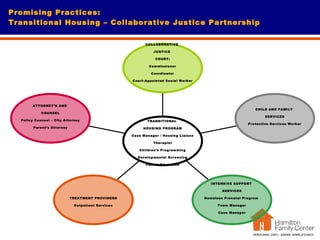
The document discusses intensive service interventions for families with disabilities. It describes who these interventions target, including those experiencing homelessness, mental health issues, substance abuse, and more. It discusses how these interventions are provided, including through transitional housing programs, permanent supportive housing, trauma-informed care, and harm reduction approaches. The core goals and philosophies of interventions include housing first, meeting families where they are, and empowering families.























































































