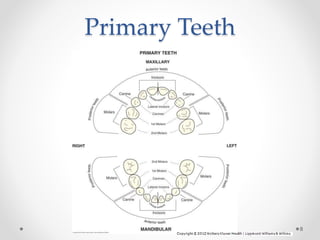
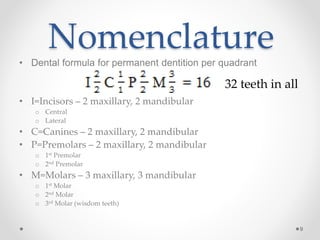
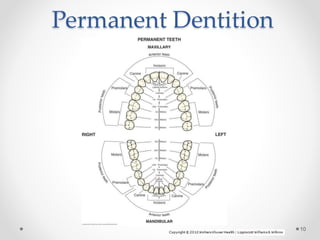
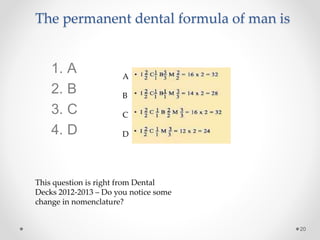
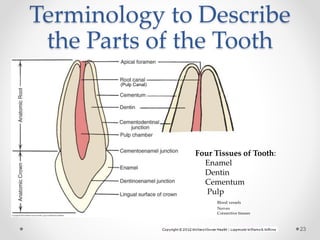
This document provides an introduction to dental terminology used to describe tooth anatomy and identification. It begins with an overview of terminology for describing the primary and permanent dentition, including dental formulas. Tooth identification systems including the Universal Numbering System and Palmer Notation are explained. Terminology is defined for identifying tooth surfaces, landmarks, and structures. Descriptions are provided for anatomical crowns and roots as well as root-to-crown ratios. Landmarks such as cusps, ridges, and line angles are defined. The document aims to familiarize students with standard dental terminology.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
