This document discusses barium swallow procedures and techniques. It provides details on:
- Barium sulfate properties and its use as a contrast agent for visualizing the gastrointestinal tract.
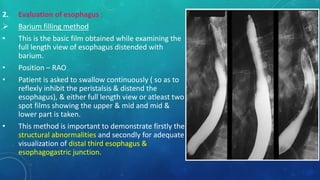
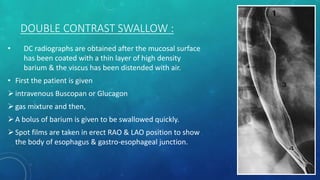
- Techniques for barium swallow exams including single and double contrast for evaluating the esophagus and surrounding anatomy.
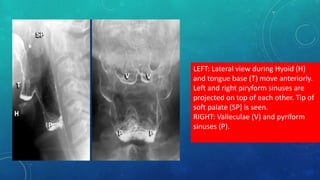
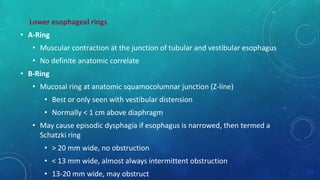
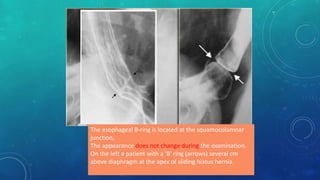
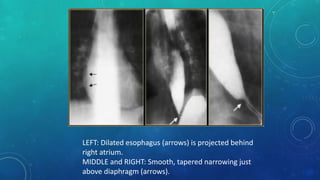
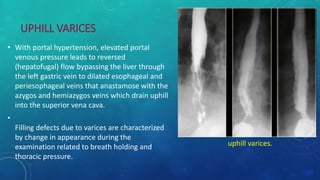
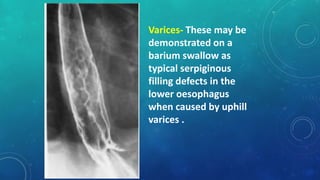
- Important anatomical landmarks visualized and potential findings such as esophageal rings, varices, and vascular impressions.
- Considerations for modifying the exam based on suspected issues like leaks or aspiration risk and conditions like motility disorders.













![COMPLETE BARIUM STUDIES Of GIT NAD [Adrian Dungu Niyimpa].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/bastudies-gitnad-220902221043-d535eaa3-thumbnail.jpg?width=640&height=640&fit=bounds)


























































