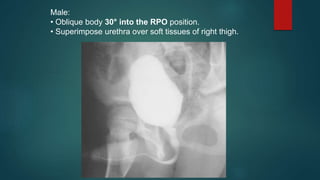
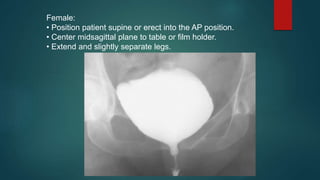
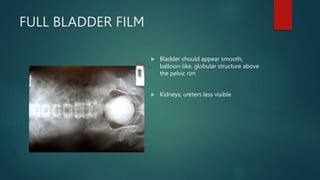
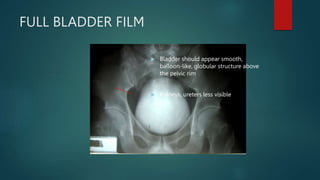
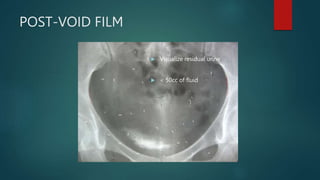
This document describes the procedure and positioning for cystourethrography and voiding cystourethrography. Cystourethrography involves injecting contrast into the bladder to visualize the bladder, ureters, and kidneys and detect abnormalities like cystitis, obstruction, vesicoureteral reflux, and bladder calculi. For males, the right posterior oblique position is used, while females are imaged in the anterior-posterior position. Voiding cystourethrography evaluates urinary retention and reflux by imaging the bladder and urethra during filling and voiding.