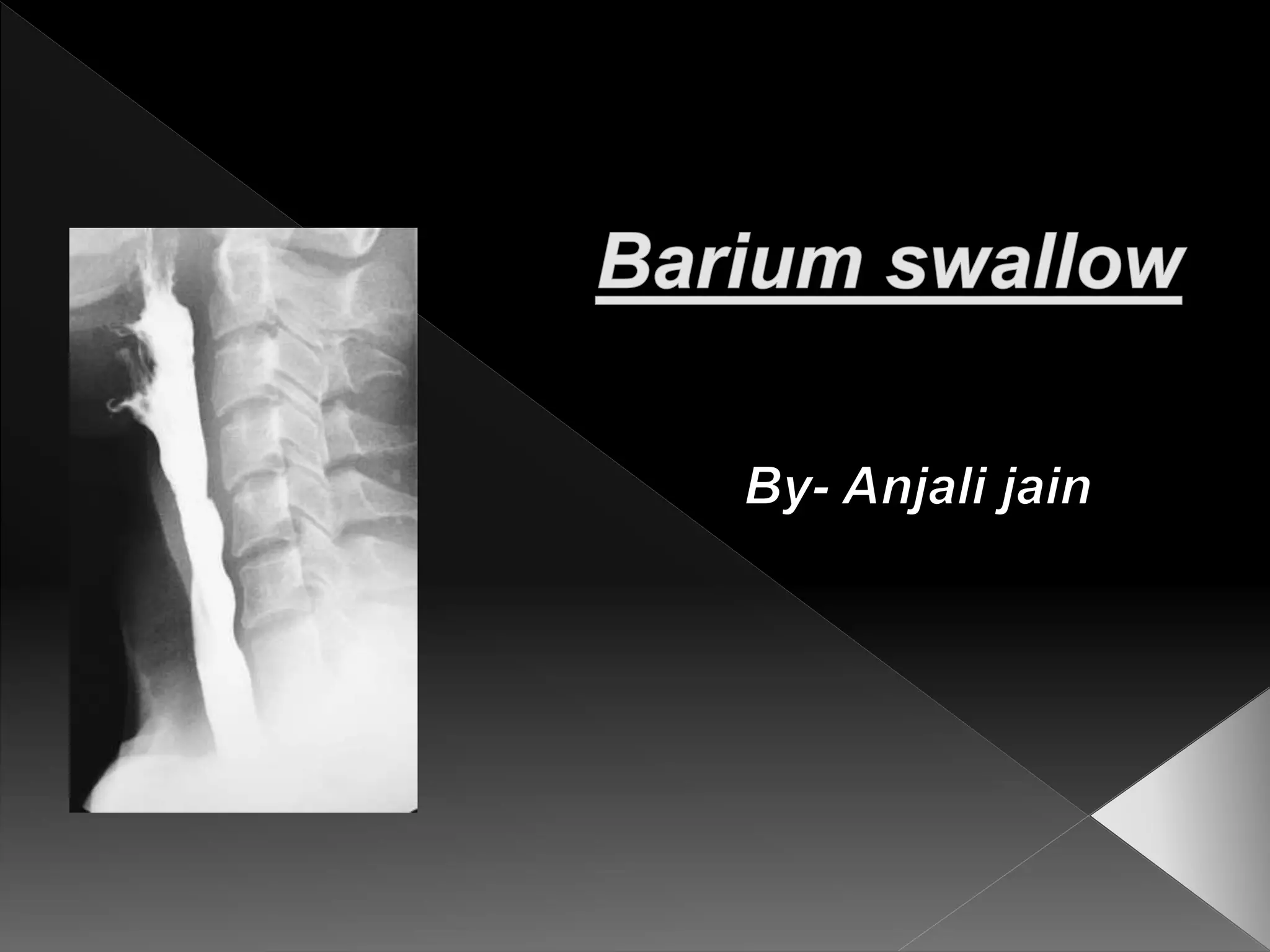
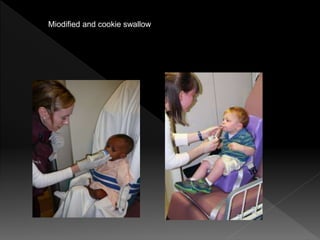
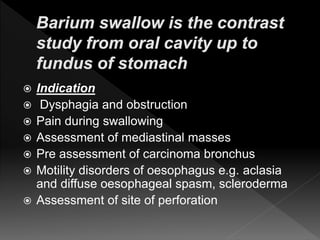
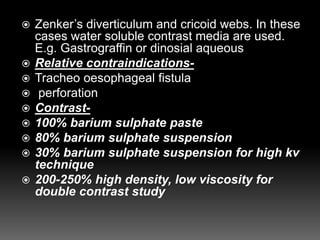
This document provides guidance on performing a modified barium swallow study to assess for dysphagia and other esophageal disorders. It describes using barium sulfate of varying densities to visualize the pharynx and esophagus during swallowing in multiple positions. Both single and double contrast techniques are outlined to optimally distend and observe the esophagus. Specific protocols are provided for evaluating various conditions like achalasia, hiatal hernia, and reflux.