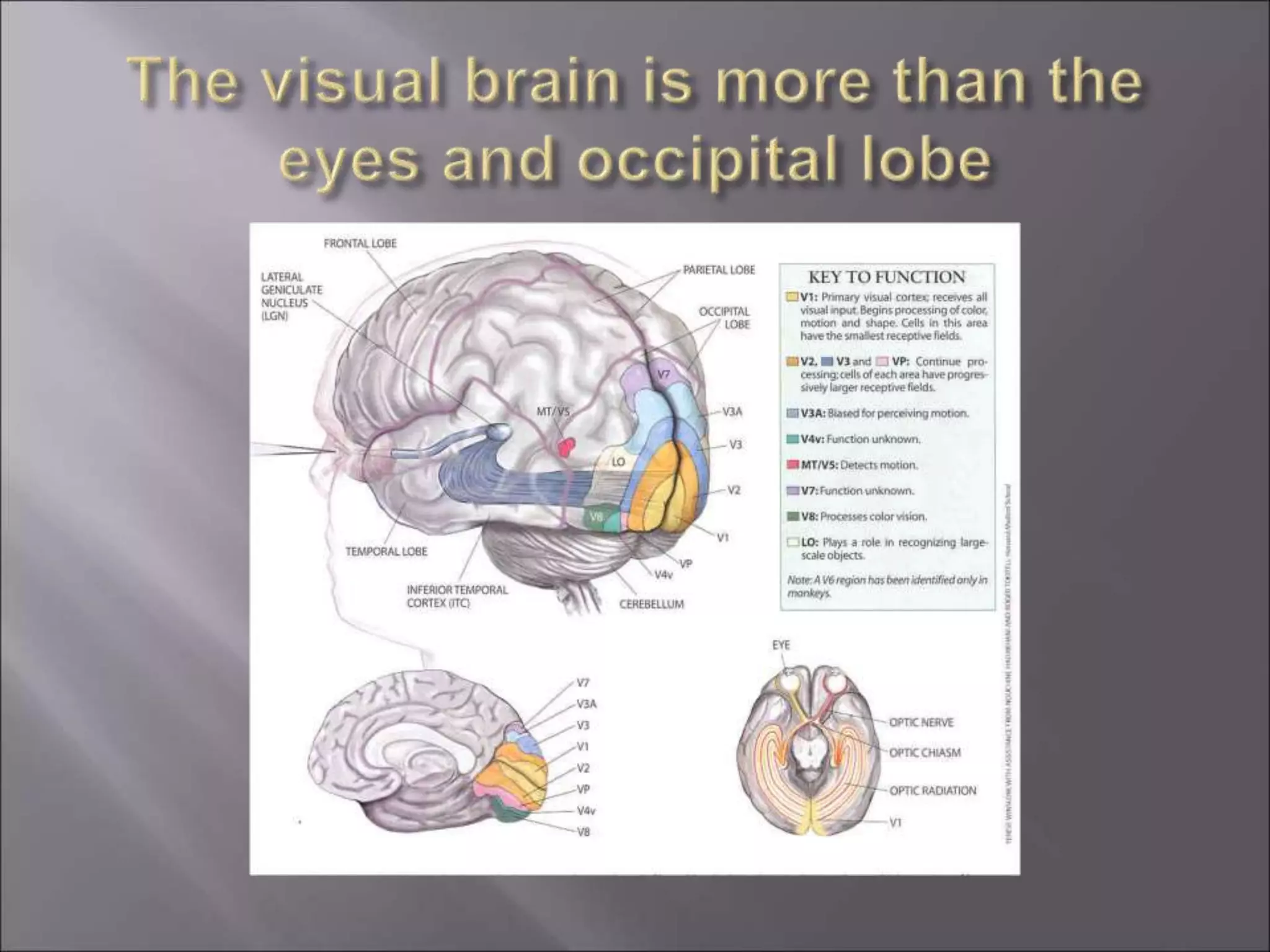
This document discusses vision syndrome, also known as binocular, accommodative, and oculomotor dysfunction (BAOD). BAOD is a common condition that affects reading and learning and often goes undetected on standard vision screenings. It involves dysfunctions in binocular control, accommodation, and oculomotor control. The document outlines signs and symptoms of BAOD, provides prevalence data, and recommends doctors evaluate for BAOD in patients with learning difficulties and refer for office-based vision therapy if needed.

























































![ContactLensComplications[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/contactlenscomplications1-230818033945-389f9be9-thumbnail.jpg?width=640&height=640&fit=bounds)
























