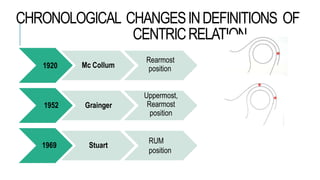
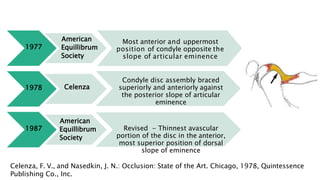
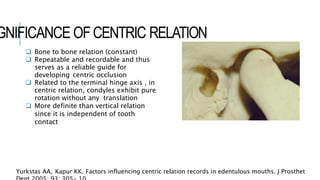
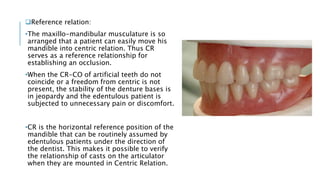
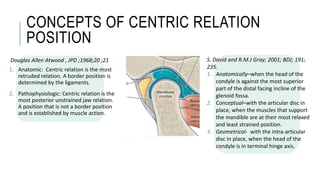
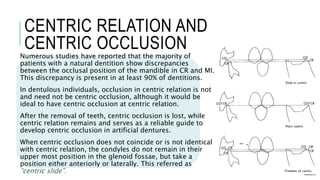
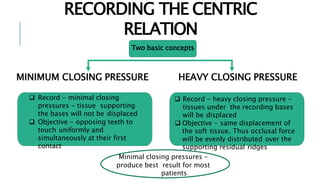
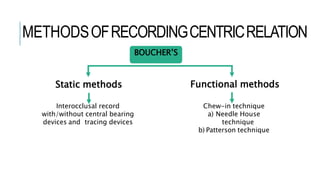
Centric relation is a controversial concept in dentistry that refers to the maxillomandibular relationship where the condyles are in their most anterior and superior position against the articular eminences, allowing purely rotary movement of the mandible. There have been many changes to the definition of centric relation over time as understanding has evolved. It is important for proper functioning and to develop centric occlusion in artificial dentures. However, accurately recording centric relation can be difficult due to various biological, psychological and mechanical factors that must be addressed. Common methods include using interocclusal records with or without central bearing devices as well as functional recording techniques.















![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)





























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















