













































![g
],
al
space is observed between the occlusal rims to ensure free
movementof stylusovertracingpadwithoutanyobstruction
or contact between opposing occlusal rims.
Figure 6: Maxillary occlusal rim with the central bearing device
(intra‑oral view)
Figure 8: Gothic arch tracing
182 The Journ
Figure 5: Vertical jaw relation
Figure 7: Mandibular occlusal rim with mounted tracer board on central
bearing device (intra‑oral view)
Figure 9: MATLAB®
software showing Gothic arch tracing and
coordinates of Gothic arch apex
Figure 5: Vertical jaw relation
Figure 7: Mandibular occlusal rim with mounted tracer board on central
bearing device (intra‑oral view)
Figure 6: Maxillary occlusal rim with the central bearing device
(intra‑oral view)
Figure 8: Gothic arch tracing
ournal of Indian Prosthodontic Society | Volume 19 | Issue 2 | April-June 2019
Figure 6: Maxillary occlusal rim with the central bearing device
(intra‑oral view)
Figure 8: Gothic arch tracing
Figure 10: Gothic arch tracing saved by software](https://image.slidesharecdn.com/centricrelationseminar-210523051300/85/Centric-relation-seminar-62-320.jpg)






































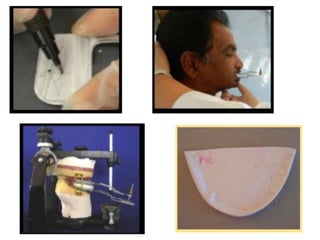









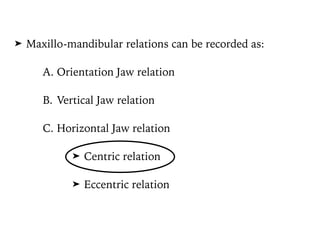
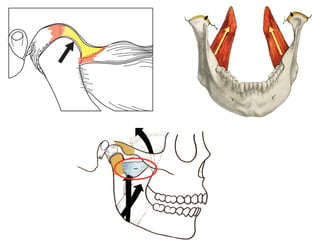
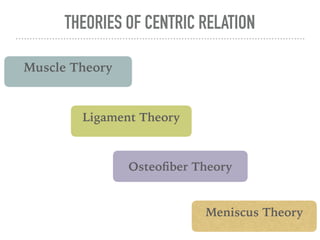
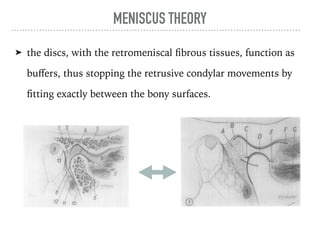
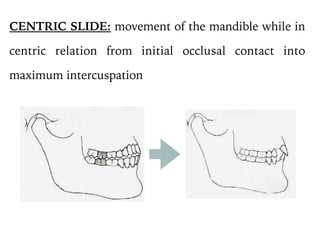
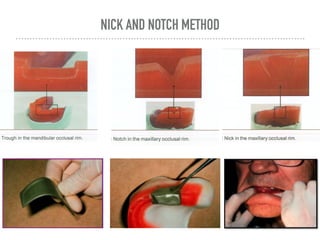
Centric relation is a maxillomandibular relationship where the condyles are positioned at the anterior-superior position against the posterior slopes of the articular eminences, allowing purely rotary movement. There are several theories regarding what determines centric relation, including muscle, ligament, osteofiber, and meniscus theories. It is important to record centric relation for complete dentures as it provides a reproducible reference position and orients the lower cast on the articulator. Common methods to record centric relation include interocclusal records, graphic tracings, and functional methods.



































































