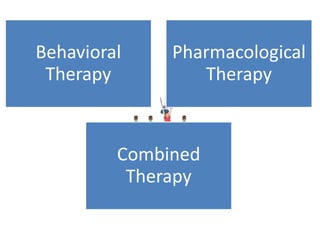
This document discusses attention deficit disorder (ADD), including its four types and their characteristics. It provides details on symptoms, causes, diagnosis criteria, and treatment approaches for ADD with hyperactivity (ADHD). Key information includes that ADHD is one of the most common childhood disorders, affecting 3-5% of school-aged children. It involves inattention, hyperactivity, and impulsivity. Treatment may involve behavioral therapy, pharmacological therapy with stimulants or non-stimulants, or a combination approach depending on the child's age. Nursing management focuses on ensuring a safe environment and developing a trusting relationship to encourage the child.