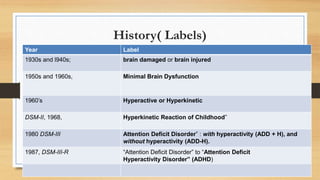
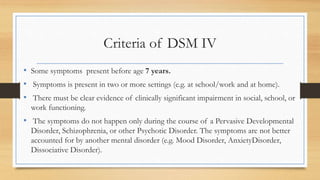
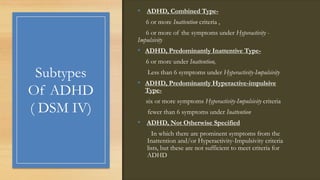
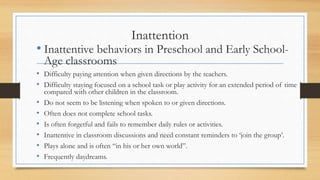
The document discusses Attention Deficit Hyperactivity Disorder (ADHD), including its definition, history of labels used, prevalence rates globally and in India, and characteristics. It provides details on the diagnostic criteria for ADHD according to the DSM-IV and DSM-V, as well as the definition and characteristics according to ICD-10. The document also discusses possible biological contributors to ADHD such as differences found in brain structure and activity levels in regions such as the prefrontal cortex, corpus callosum, striatum, and cerebellum.

















































![ADHD (best)]](https://cdn.slidesharecdn.com/ss_thumbnails/bykhaihojoshuagabriel1-1234763718979961-1-thumbnail.jpg?width=640&height=640&fit=bounds)