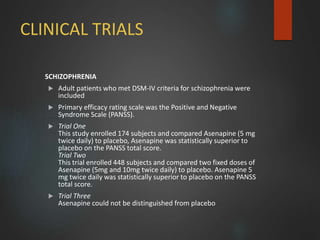
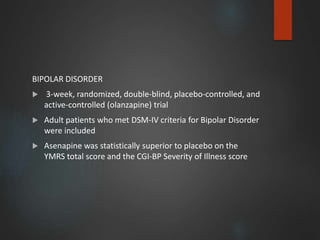
1) Asenapine and agomelatine are drugs used to treat schizophrenia, bipolar disorder, and major depressive disorder. Asenapine is an antipsychotic while agomelatine is an antidepressant with a novel mechanism of action targeting melatonin receptors.
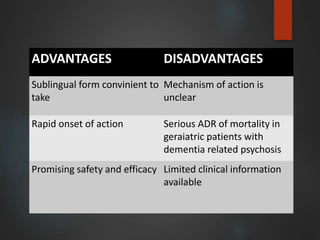
2) Both drugs have advantages like rapid onset of action and promising safety profiles. However, they also have limitations and warnings. Asenapine is associated with increased mortality in elderly patients with dementia. Agomelatine requires dose adjustment in patients with hepatic impairment.
3) The document provides details on the pharmacology, pharmacokinetics, clinical trials, dosing, precautions and drug interactions of asenap





![Chemistry
Synthetic analog of the hormone melatonin
N-[2-(7-methoxynaphthalen-1-yl) ethyl] acetamide](https://image.slidesharecdn.com/asenapineagomelatine-170209104220/85/Asenapine-agomelatine-36-320.jpg)