

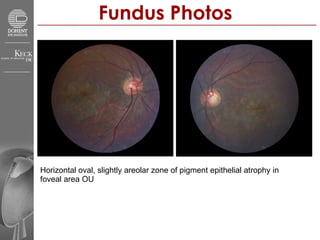
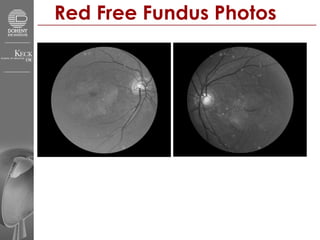
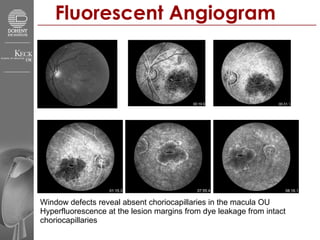
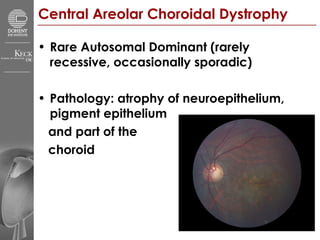
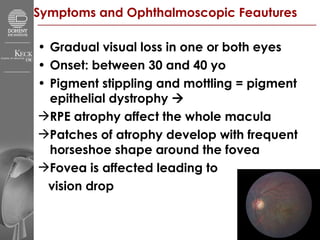
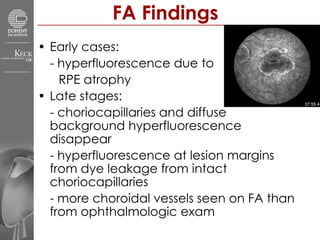

A 31-year-old Vietnamese male presented with gradual decreased vision in both eyes since adolescence. Examination revealed pigment epithelial atrophy in the foveal area of both eyes. Fluorescein angiography showed window defects from absent choriocapillaries in the macula of both eyes. He was diagnosed with central areolar choroidal dystrophy, a rare autosomal dominant condition characterized by atrophy of the neuroepithelium, pigment epithelium, and part of the choroid resulting in gradual visual loss.














































































