


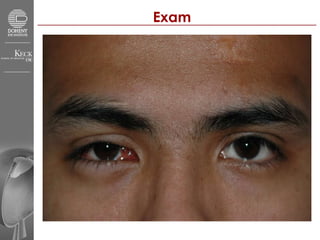
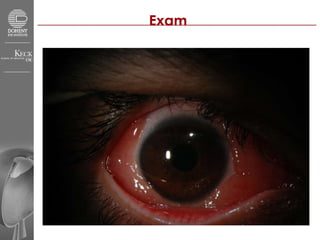


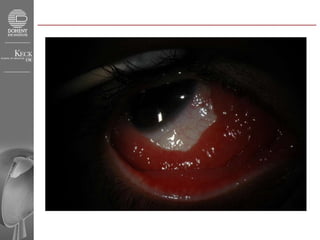


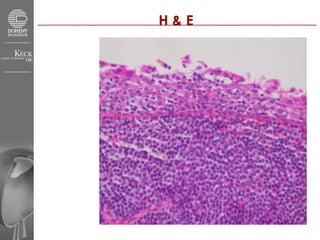

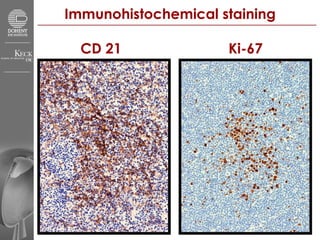

A 24-year-old man presented with an enlarging growth in his right eye that had been progressively growing larger over 8 months since being kicked in the eye. Examination found a growth in the right eye with full vision and eye movement. Biopsy of the growth found characteristics of mucosa-associated lymphoid tissue (MALT) lymphoma. MALT lymphoma can occur in the conjunctiva and has a generally favorable prognosis when treated locally. Further testing will be done to evaluate if the cancer is localized or has spread systemically.














































































