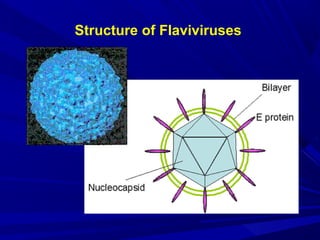
Arboviruses, or arthropod-borne viruses, are viruses that can be transmitted to humans by arthropod vectors such as mosquitoes and ticks. They infect susceptible vertebrate hosts and are maintained in nature through transmission between hosts by hematophagous arthropods. Approximately 80 arboviruses are known to cause human disease. Common arboviruses include those that cause dengue, yellow fever, Japanese encephalitis, West Nile fever, and chikungunya. They are often associated with diseases ranging from mild febrile illness to severe encephalitis or hemorrhagic fever. Arboviruses are classified into families including Togaviridae, Flavivir



























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)