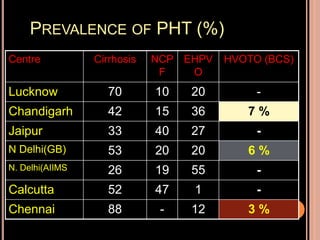
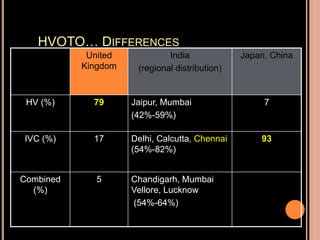
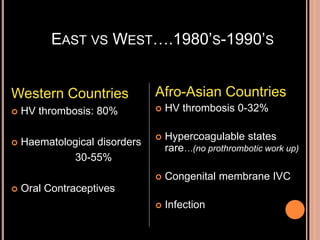
This document summarizes the work of Dr. N Madanagopalan regarding Budd-Chiari syndrome (BCS) from 1978-1996. It highlights that Dr. Madanagopalan made major contributions to understanding the epidemiology, clinical presentation, investigations and management of BCS. Through angiographic and surgical studies conducted with collaborators, he helped establish the patterns and treatment of hepatic vein outflow tract obstruction in India. His work demonstrated differences from Western countries and identified congenital abnormalities as a major cause. This laid the foundation for endovascular treatments now used.