Downloaded 27 times


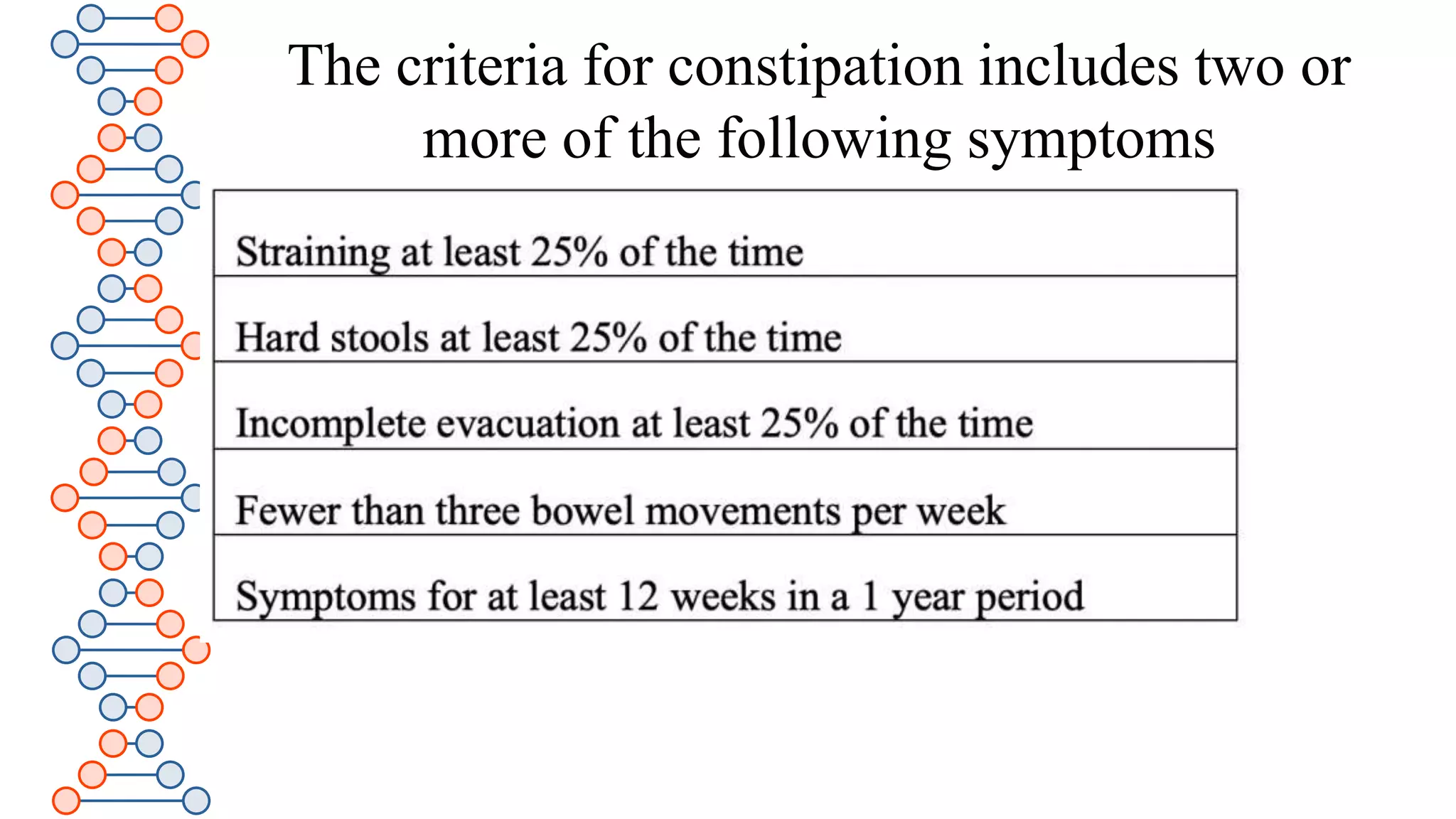
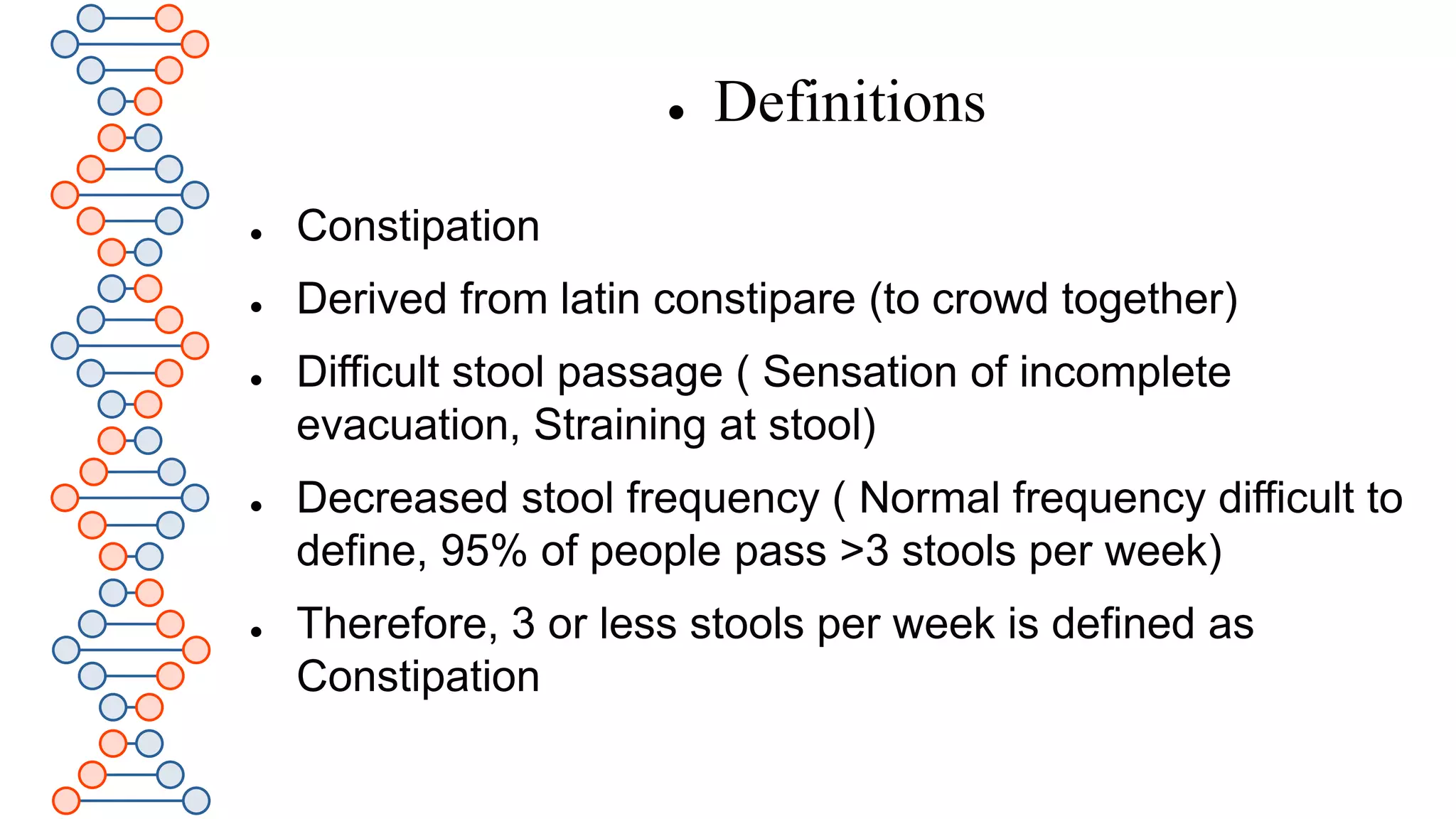
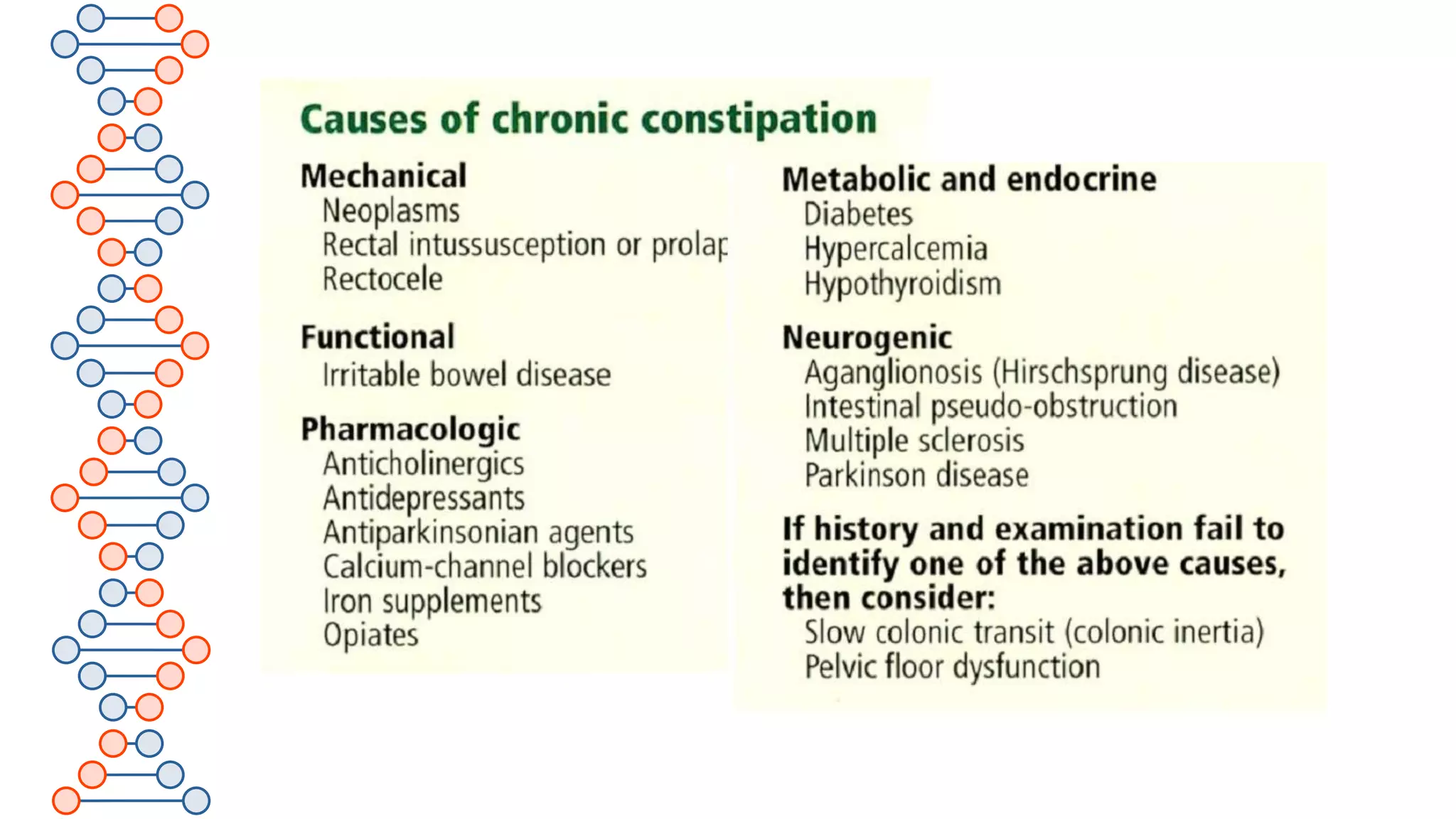
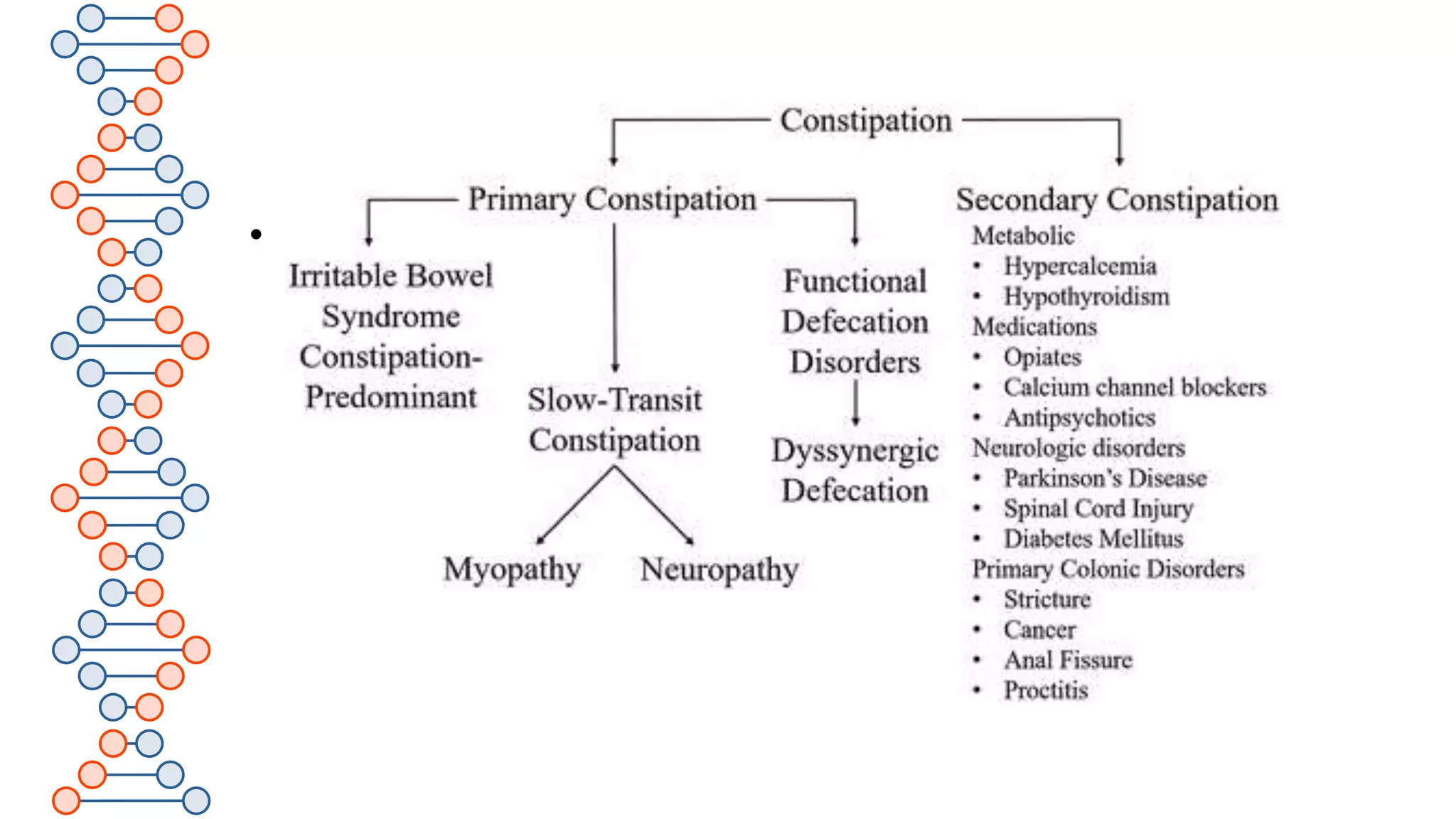
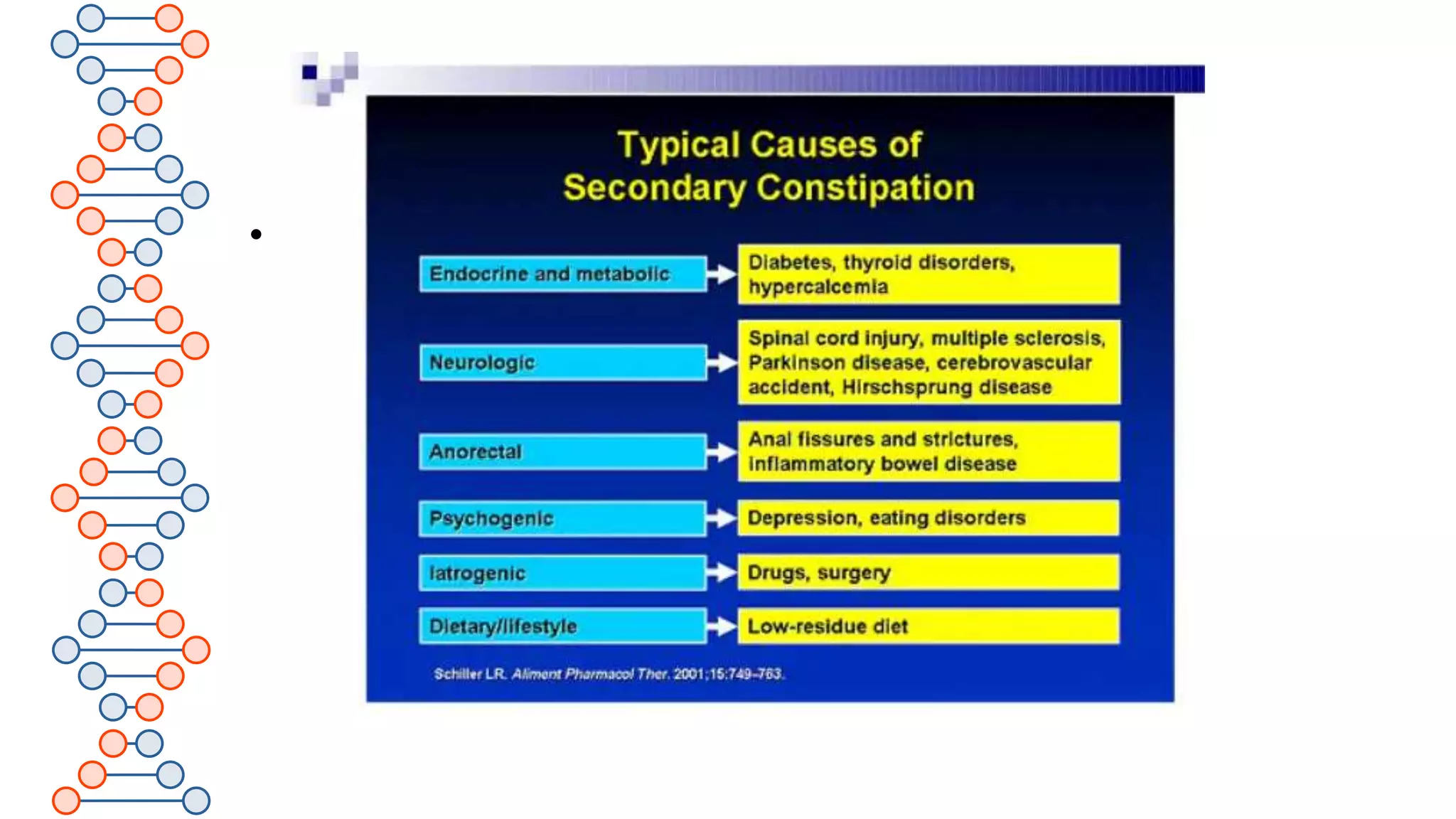















Chronic constipation is a worldwide problem that can be primary or secondary. It involves two or more symptoms including difficult stool passage, decreased stool frequency of less than three times per week, and a sensation of incomplete evacuation or straining. The causes of constipation are complex and multifaceted. Treatment involves dietary changes with increased fluids and fiber intake, fiber supplements, laxatives, prokinetics, pelvic floor rehabilitation, sacral nerve stimulation or anorectal surgery depending on the severity and underlying cause. Complications can include hemorrhoids, anal fissures, rectal bleeding and impaction.


















































































