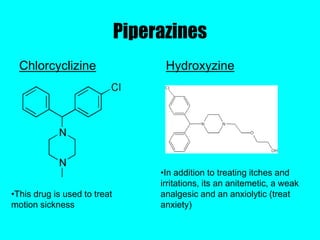
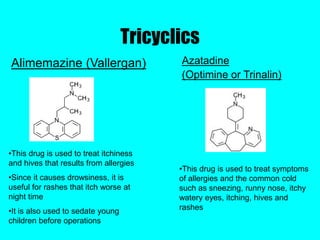
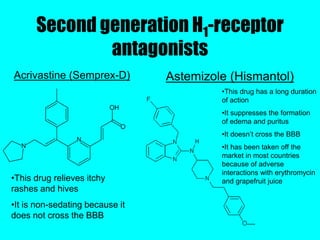
Antihistamines are drugs that reduce or eliminate the effects of histamine, which is released during allergic reactions. There are several classes of antihistamines including first generation, second generation, and third generation. First generation antihistamines are effective but cause more side effects like sedation due to their ability to cross the blood brain barrier. Newer generations have been developed with greater selectivity for peripheral histamine receptors, resulting in fewer side effects. Research continues on developing more selective antihistamines and exploring the anti-inflammatory properties and potential for new treatments.

































































![lecture-4 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture-4autosaved-230730161044-605918a6-thumbnail.jpg?width=640&height=640&fit=bounds)














































