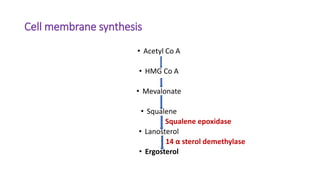
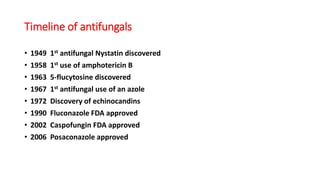
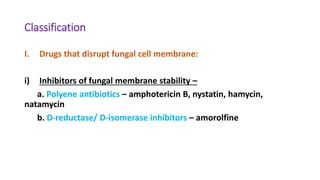
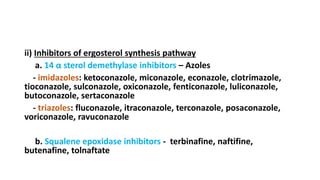
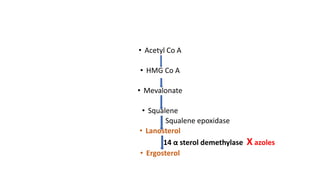
This document summarizes various antifungals, including their mechanisms of action, classifications, and indications. It discusses polyene antibiotics like amphotericin B and nystatin, azoles like fluconazole and itraconazole that inhibit ergosterol synthesis, squalene epoxidase inhibitors like terbinafine, echinocandins that disrupt the fungal cell wall, and other antifungals. It provides a timeline of antifungal development and covers the pharmacology, spectrum of activity, dosing, and adverse effects of major antifungal classes.