Downloaded 92 times
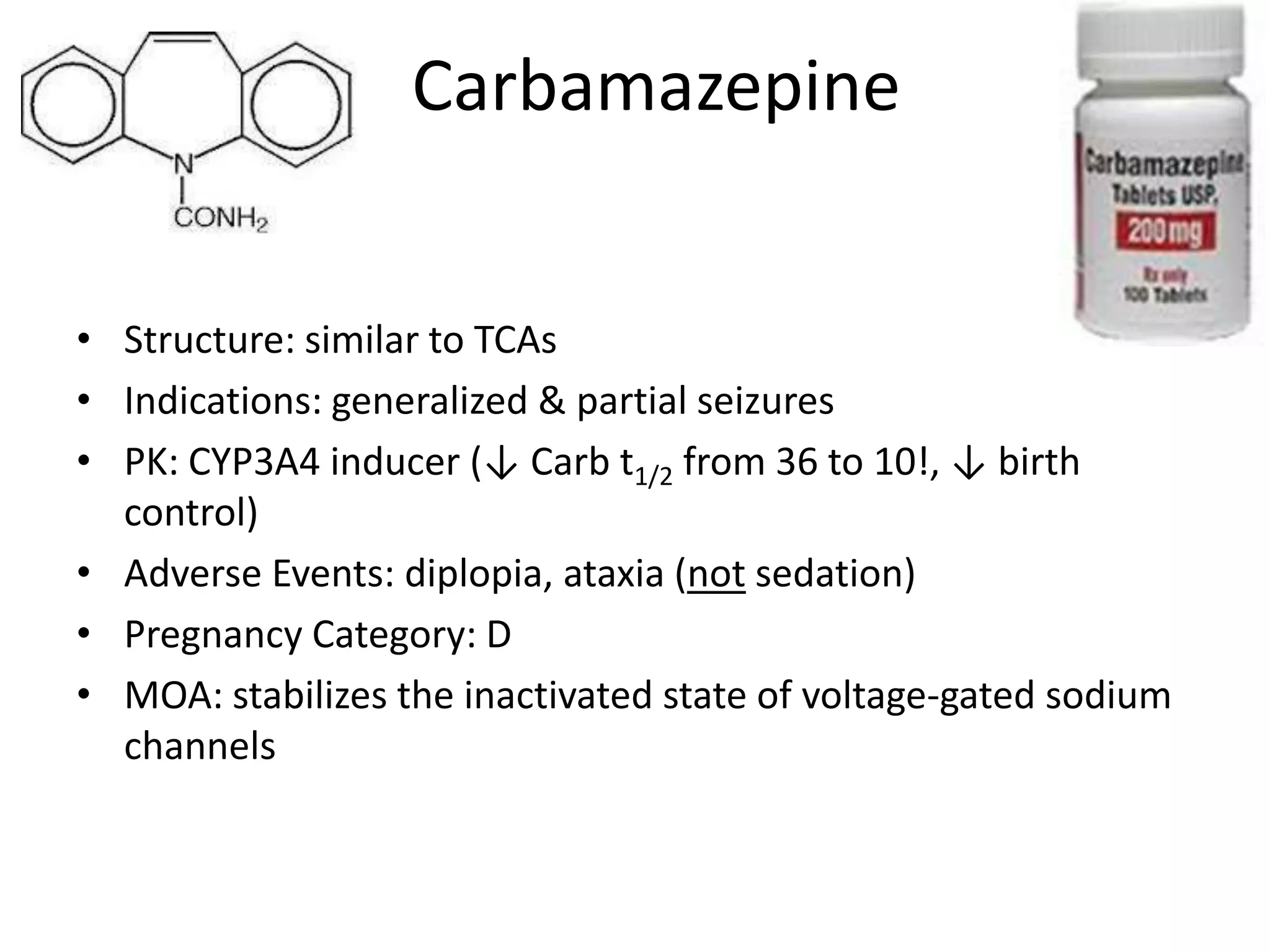
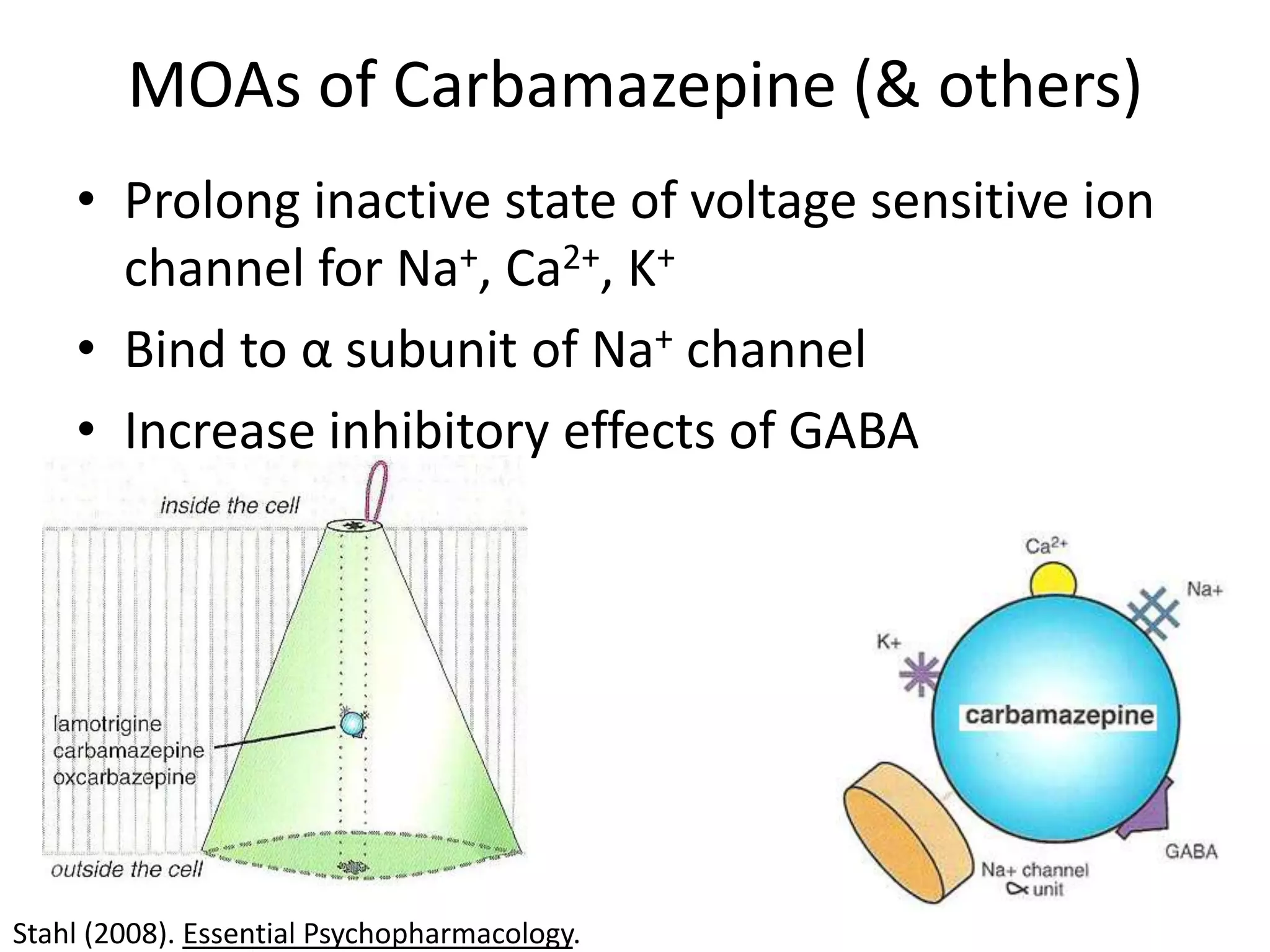
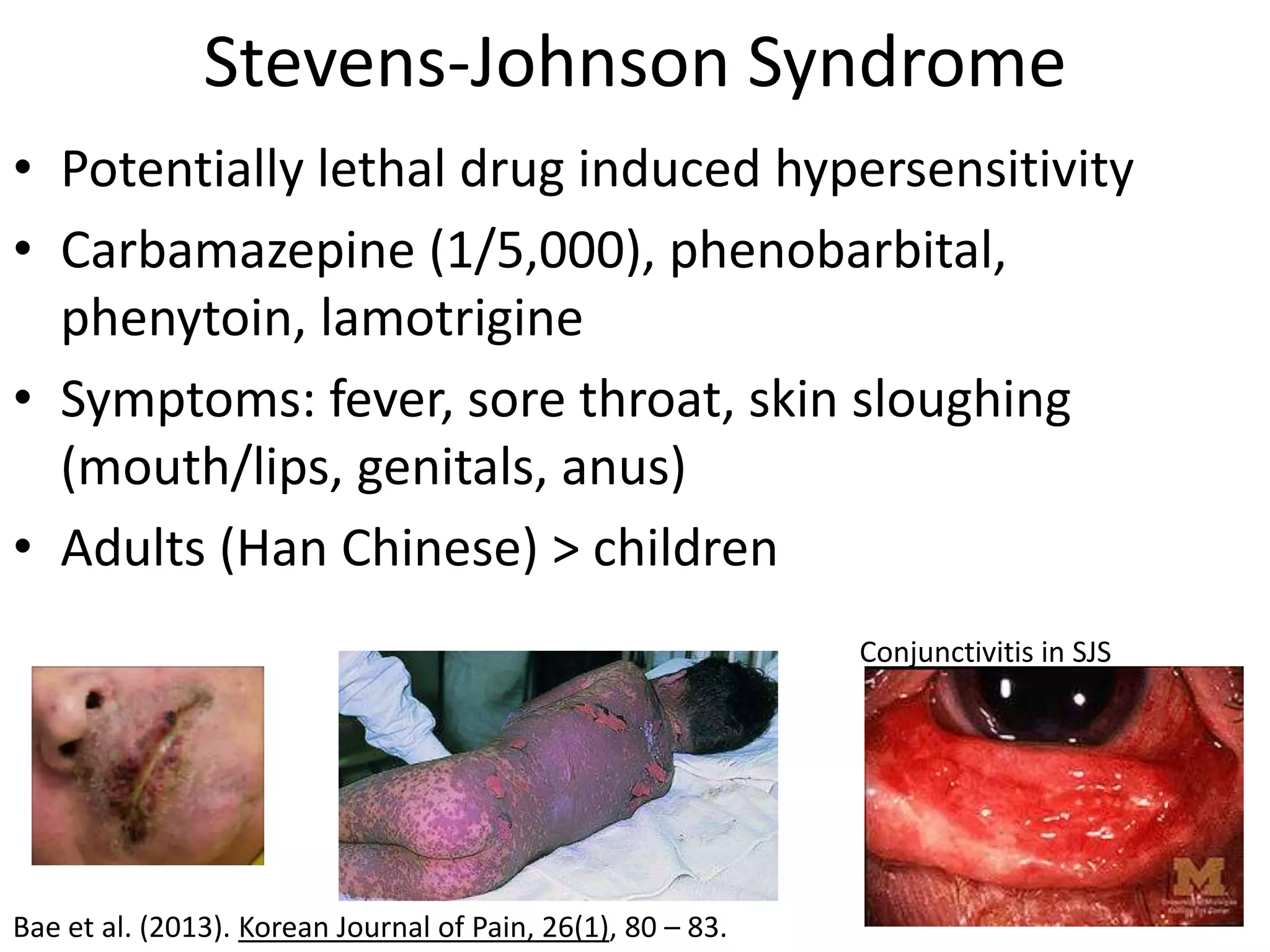
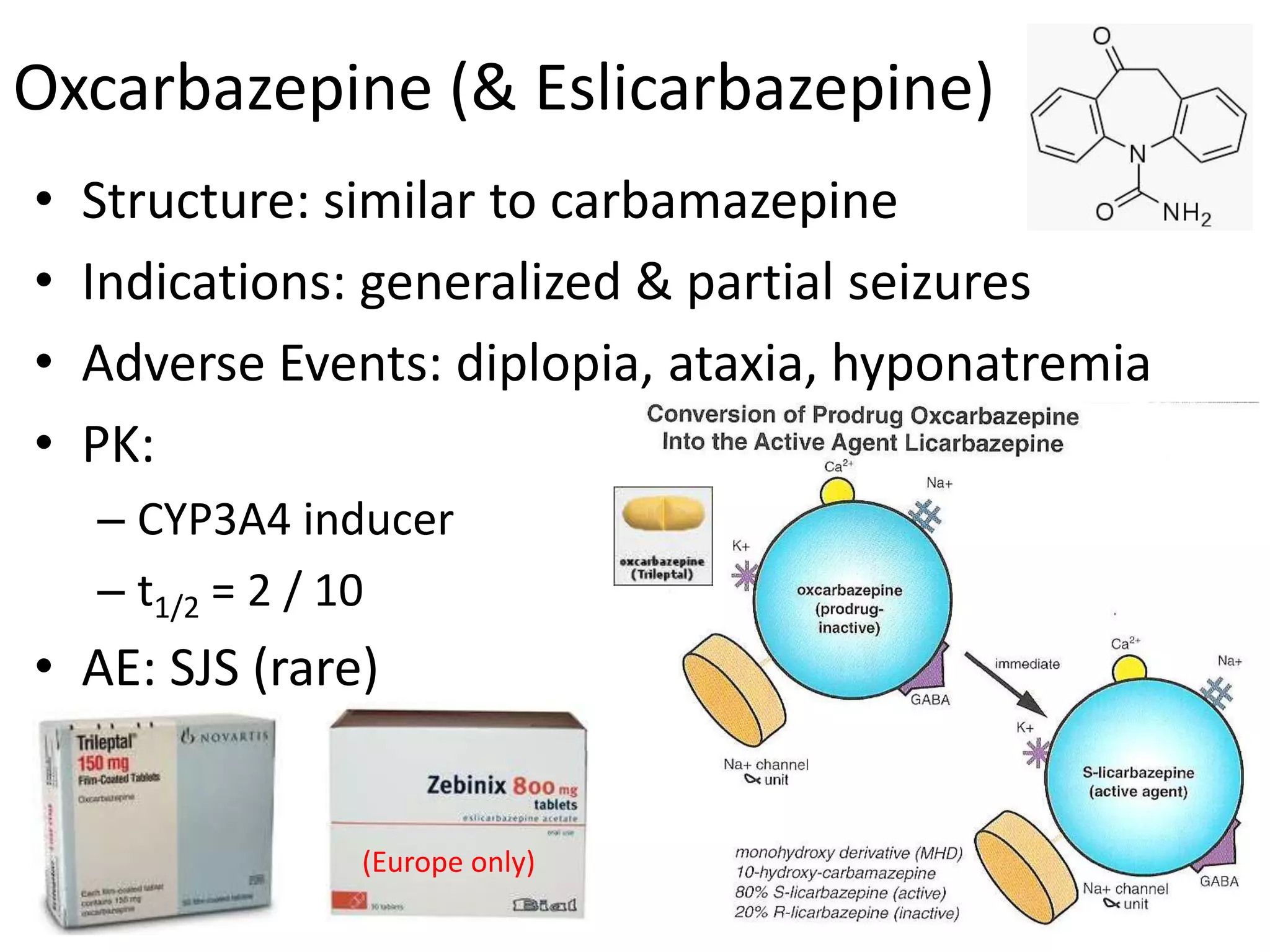
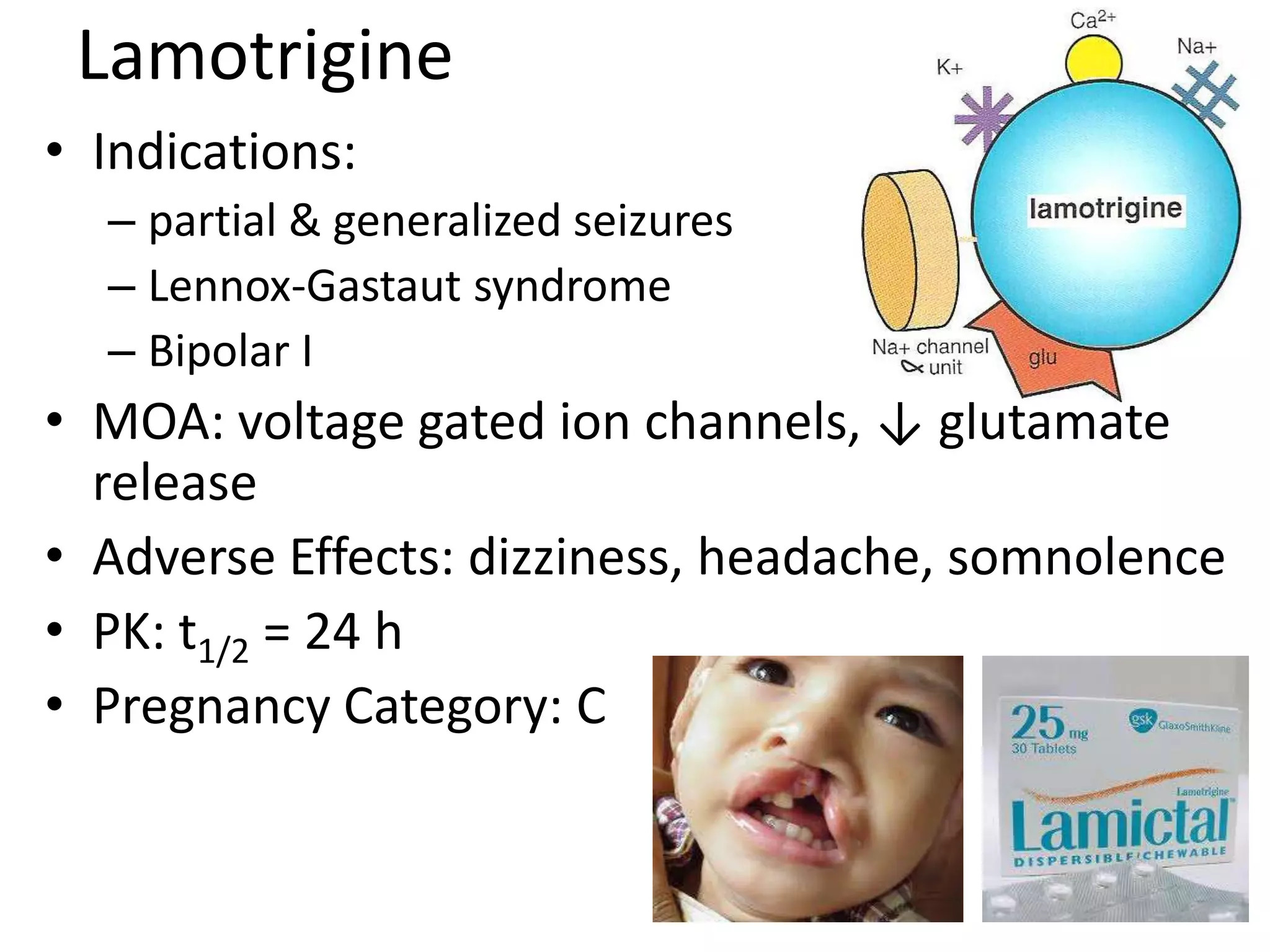
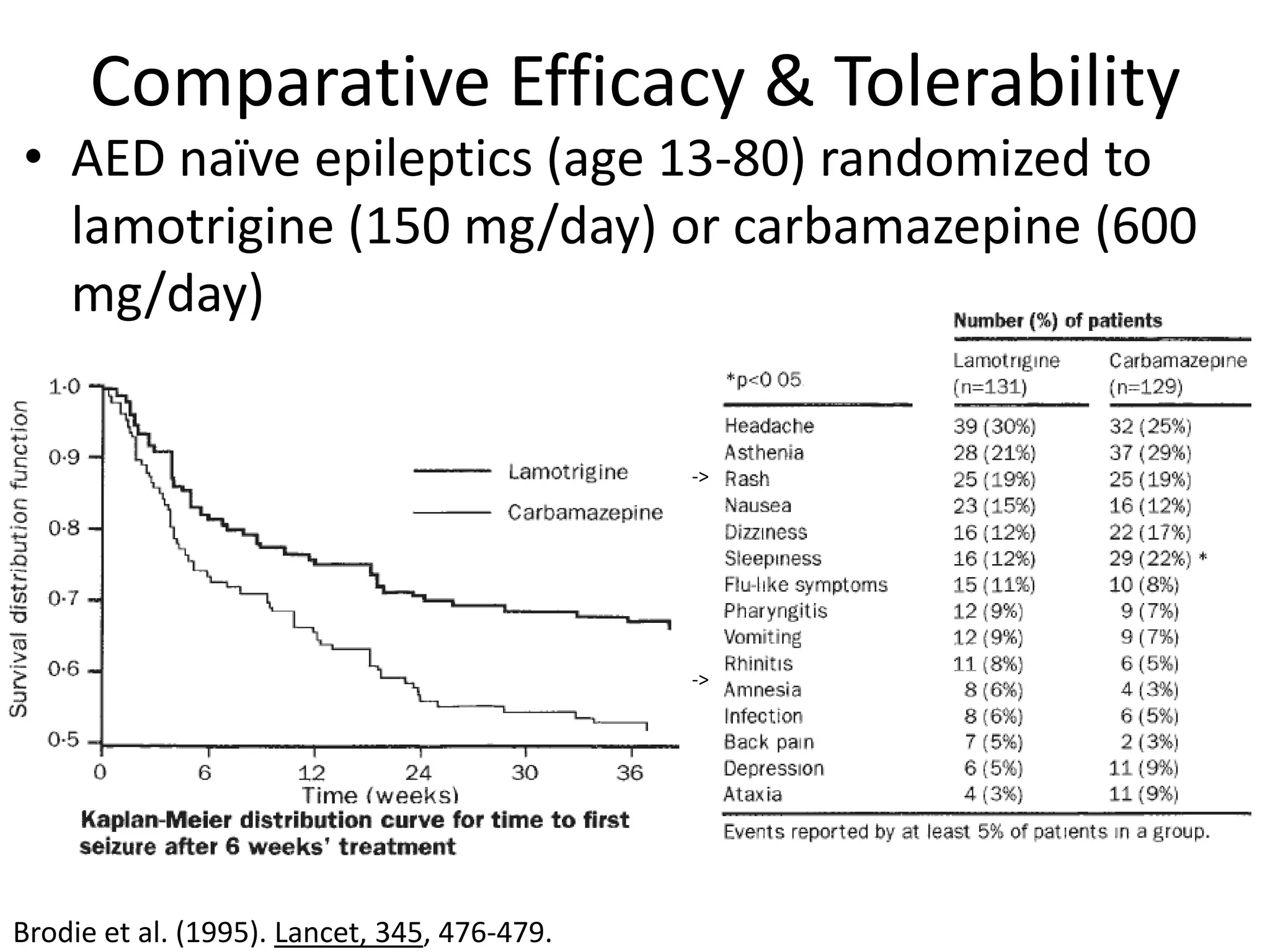
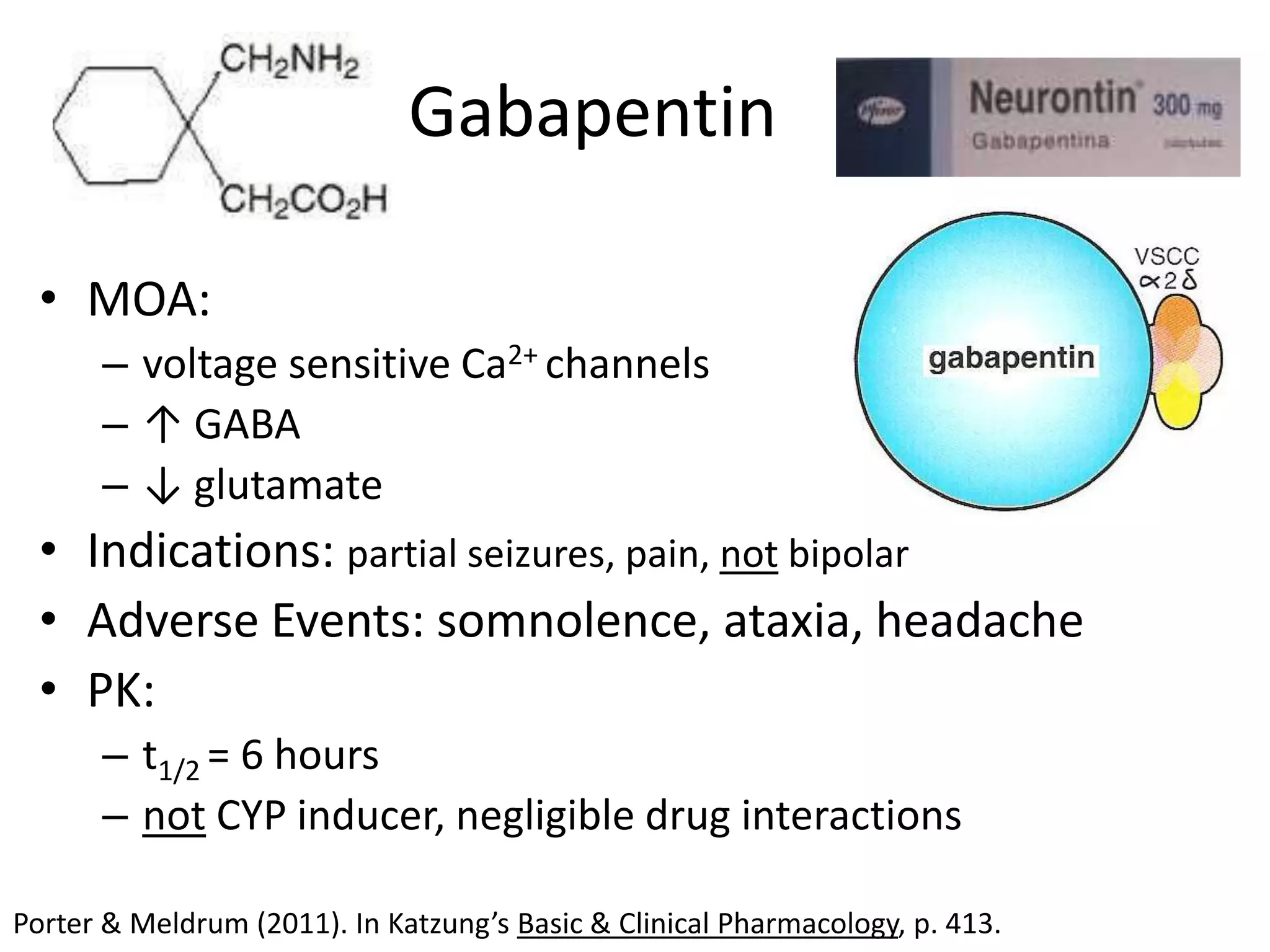
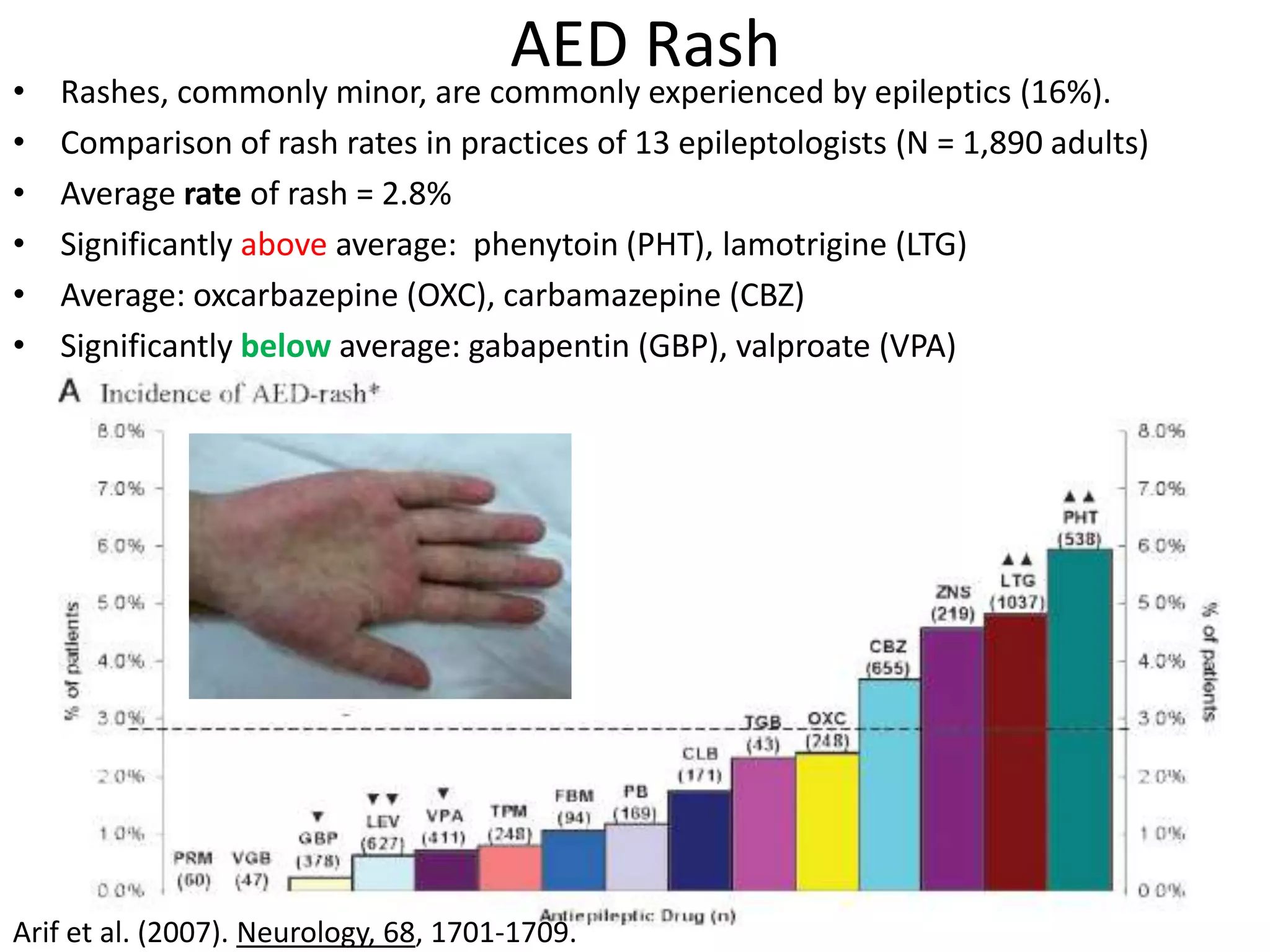
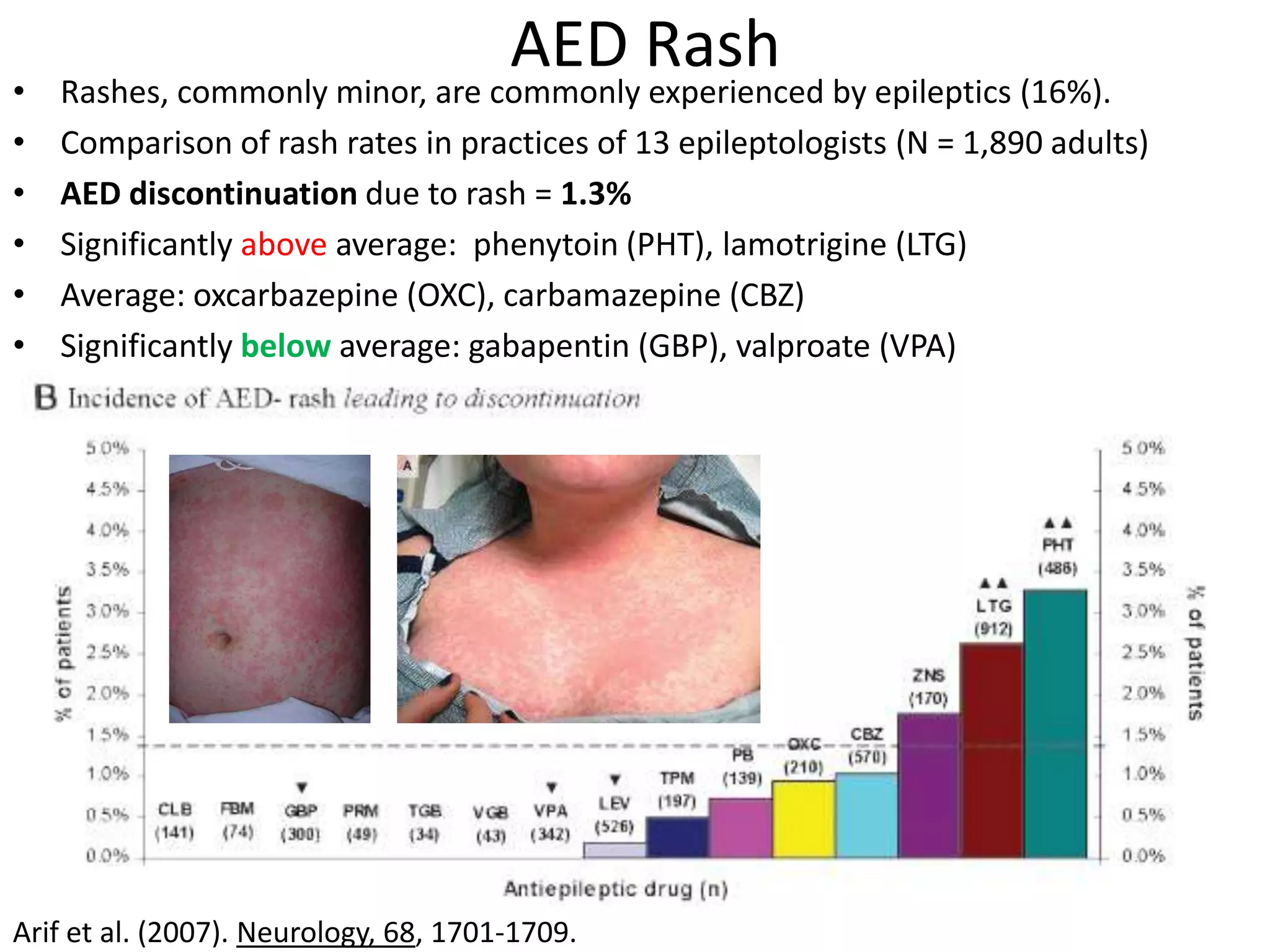
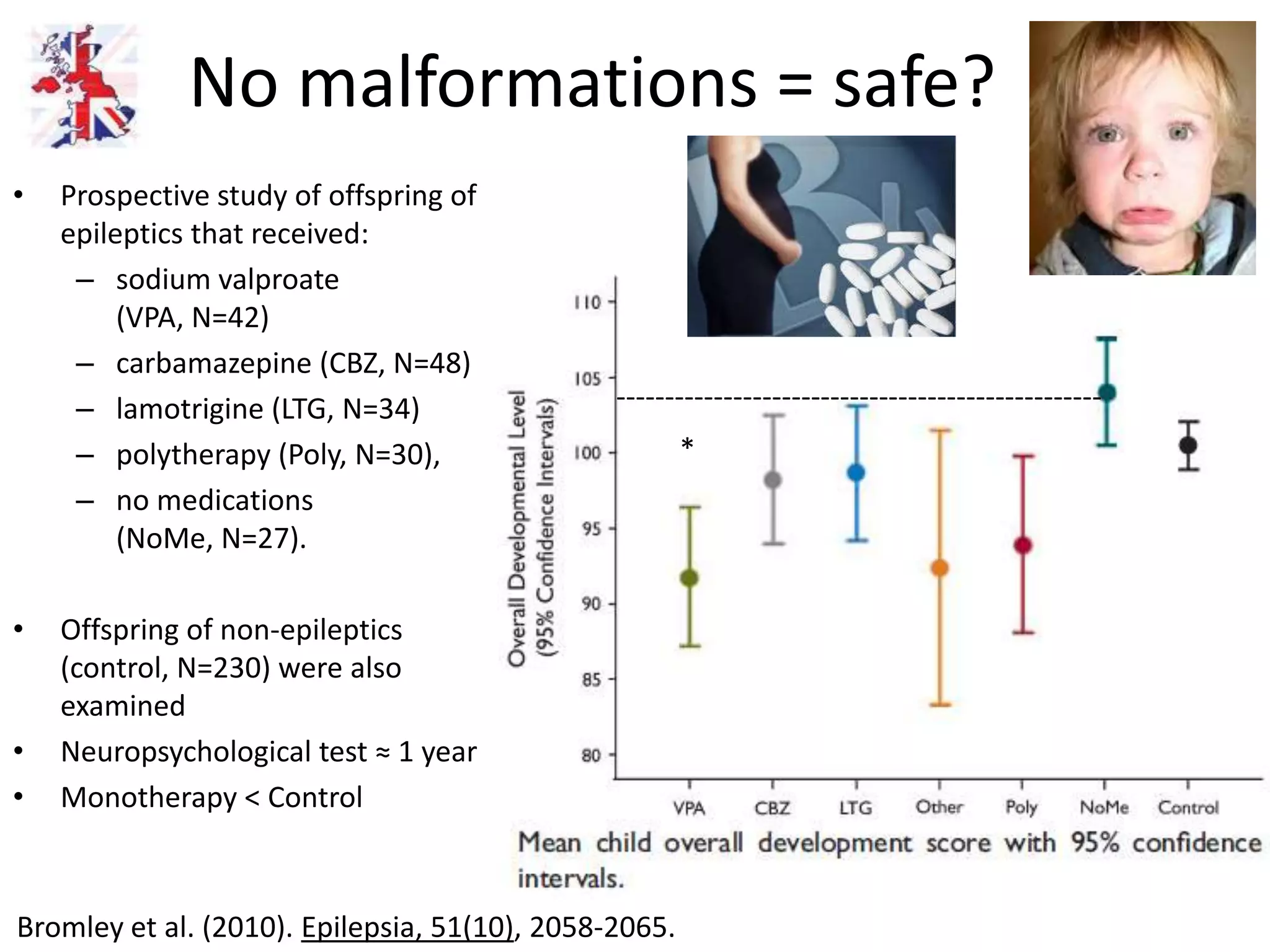
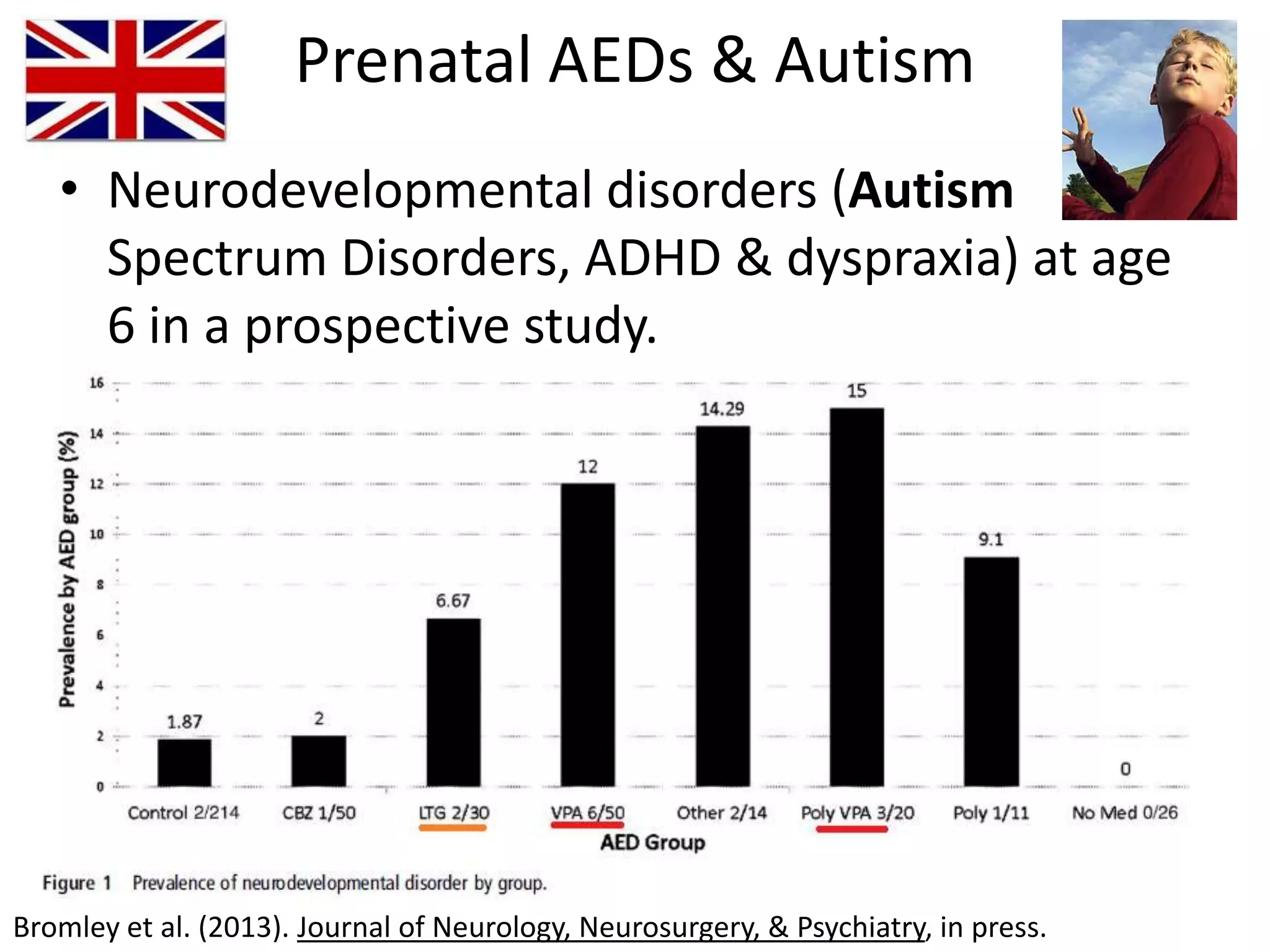
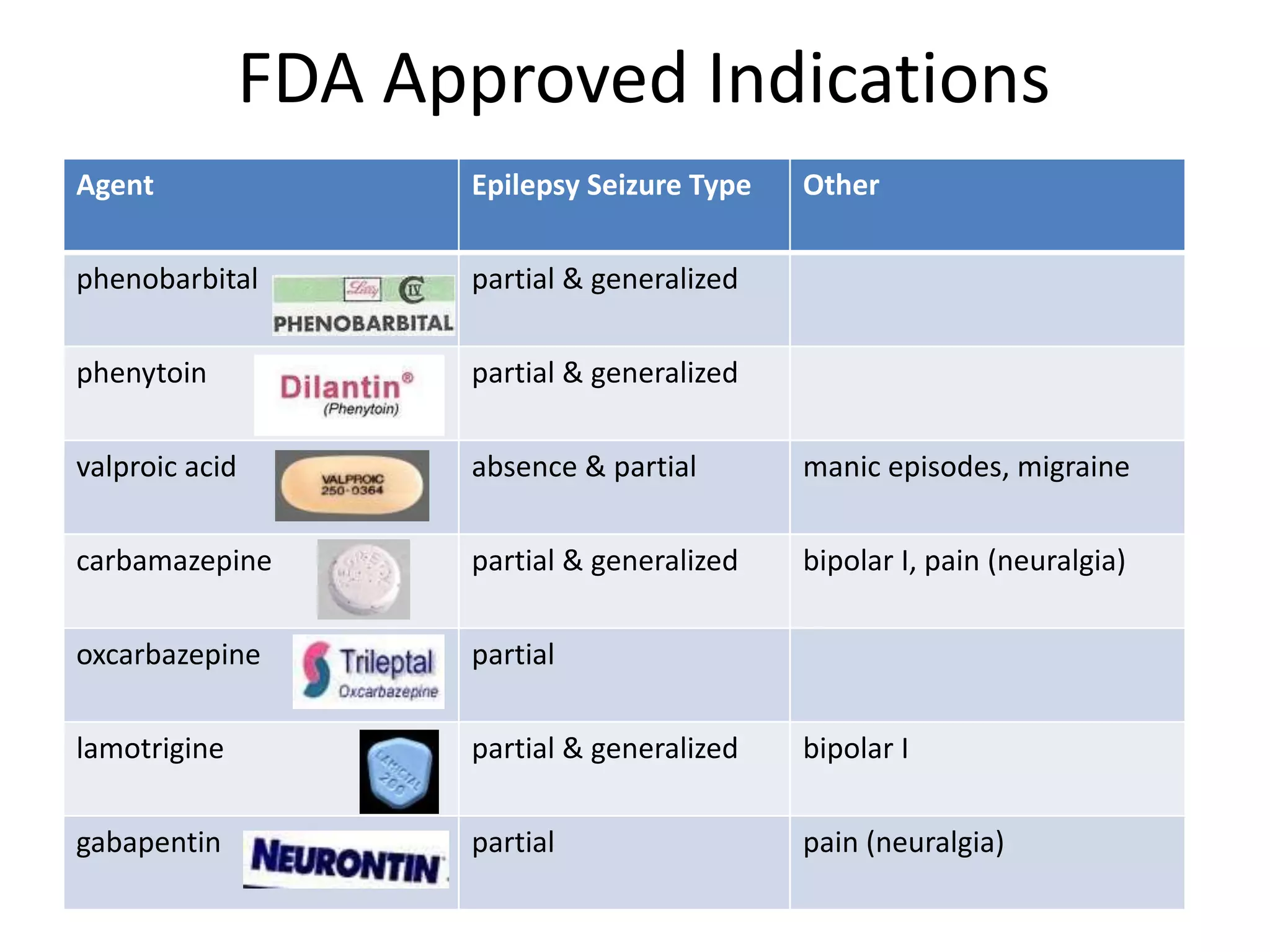

This document discusses various anticonvulsants, focusing on their mechanisms of action, indications, side effects, and pharmacokinetics. It highlights the differences in adverse events associated with different antiepileptic drugs (AEDs), particularly noting the occurrence of rashes and the implications of prenatal exposure. Additionally, it mentions the higher suicide rates among epileptics and emphasizes that while newer AEDs may be better tolerated, efficacy improvements are limited, leading to common use of polytherapy.























































































