Downloaded 643 times

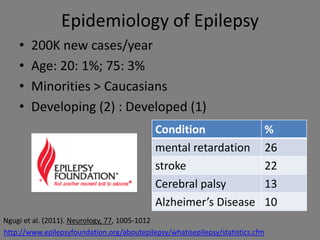
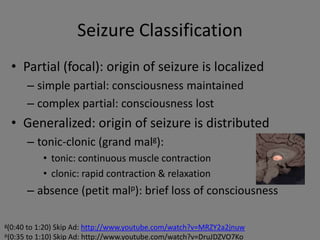
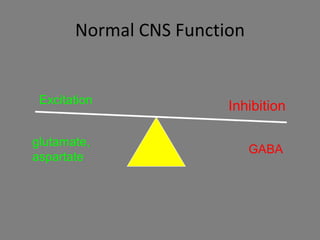
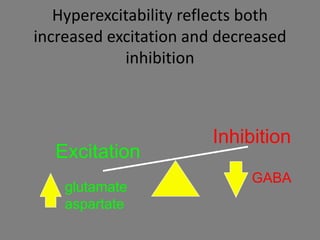
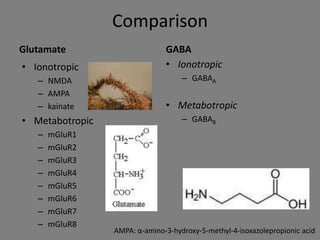
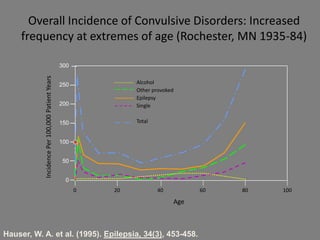
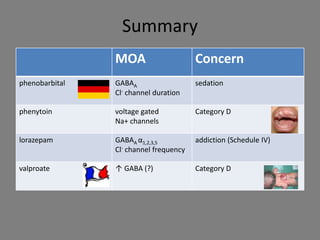
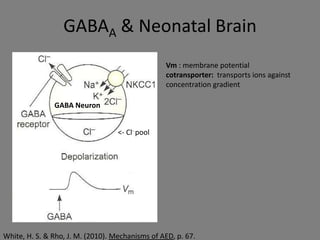
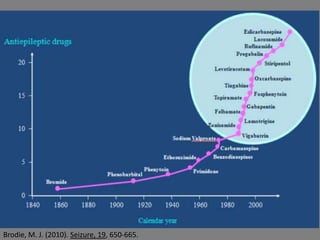

This document provides an overview of anticonvulsants, their mechanisms of action, and the neurochemistry of seizures. It discusses the classification of seizures, the history of antiepileptic drugs (AEDs), and their various adverse effects and uses. Key points include the epidemiology of epilepsy and the increased seizure incidence at extreme ages.























































































