Downloaded 89 times
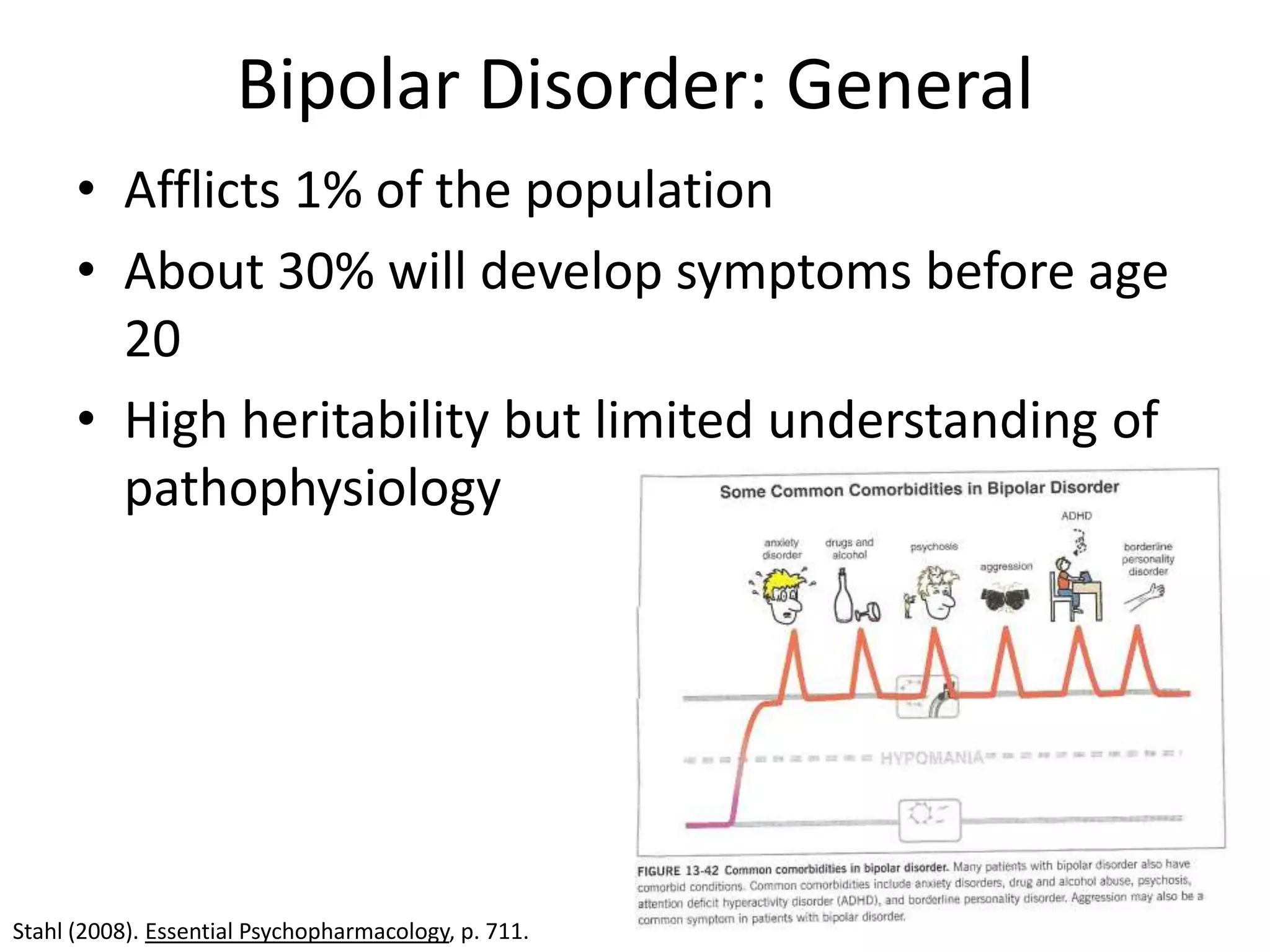
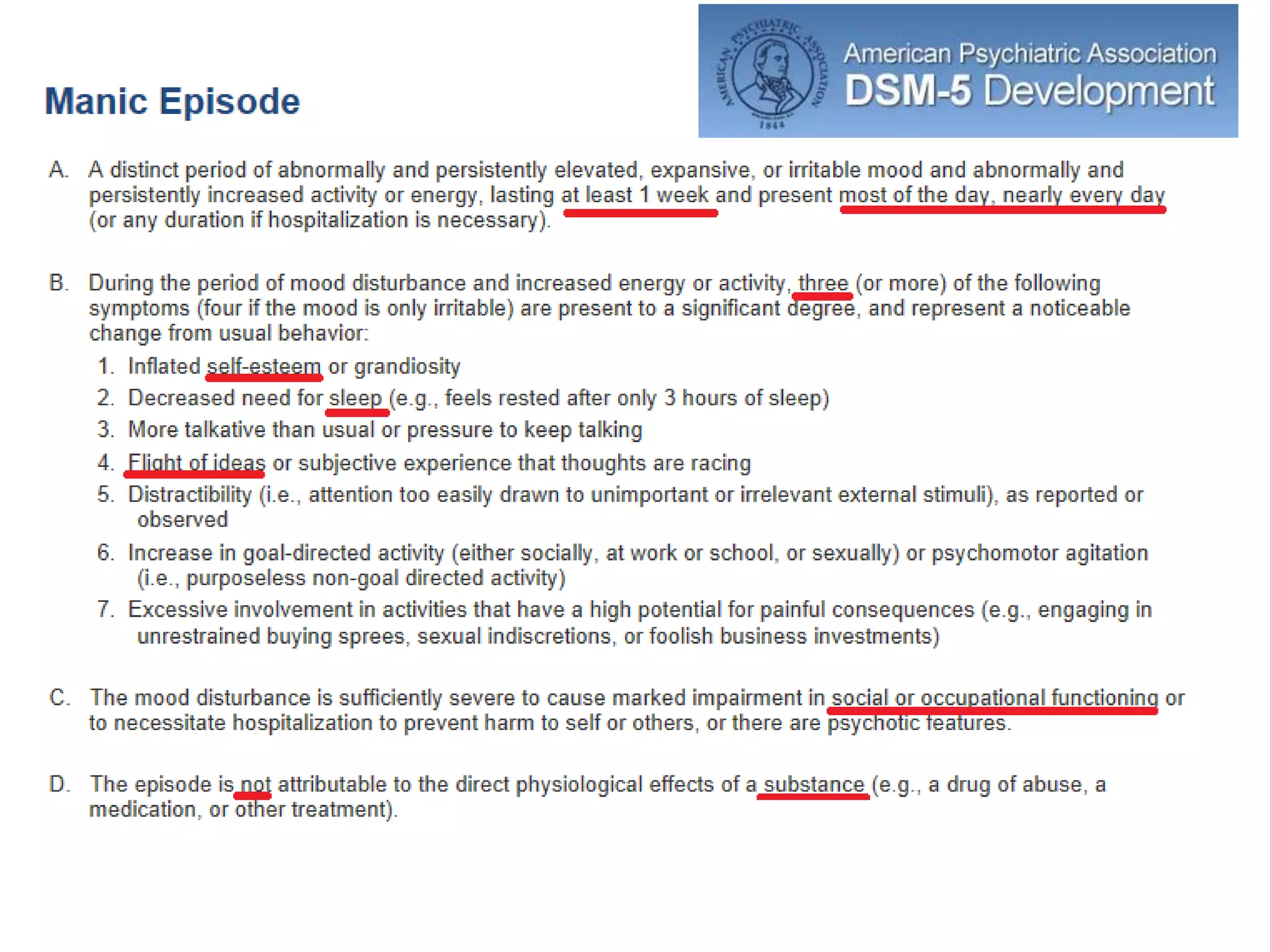
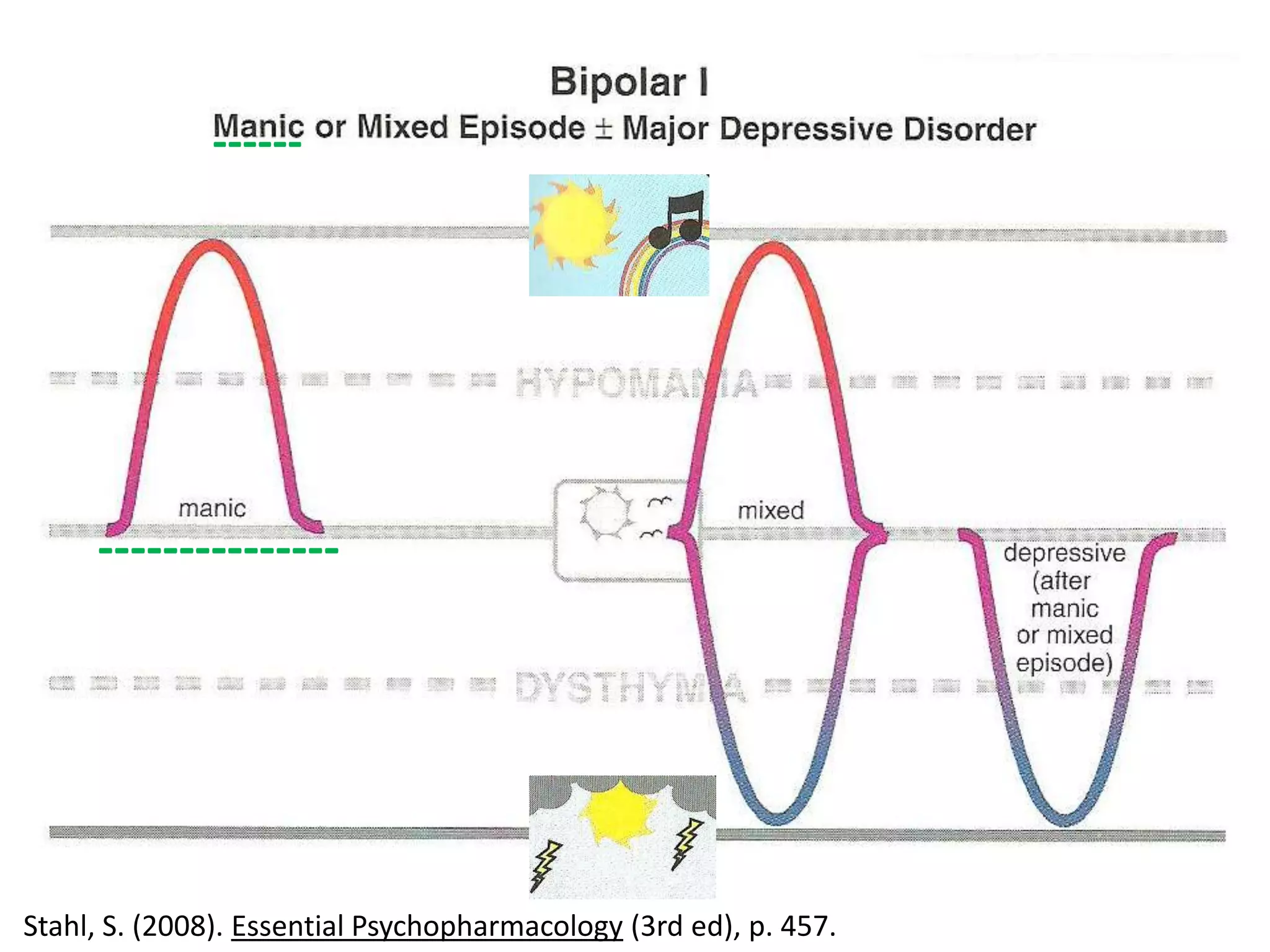
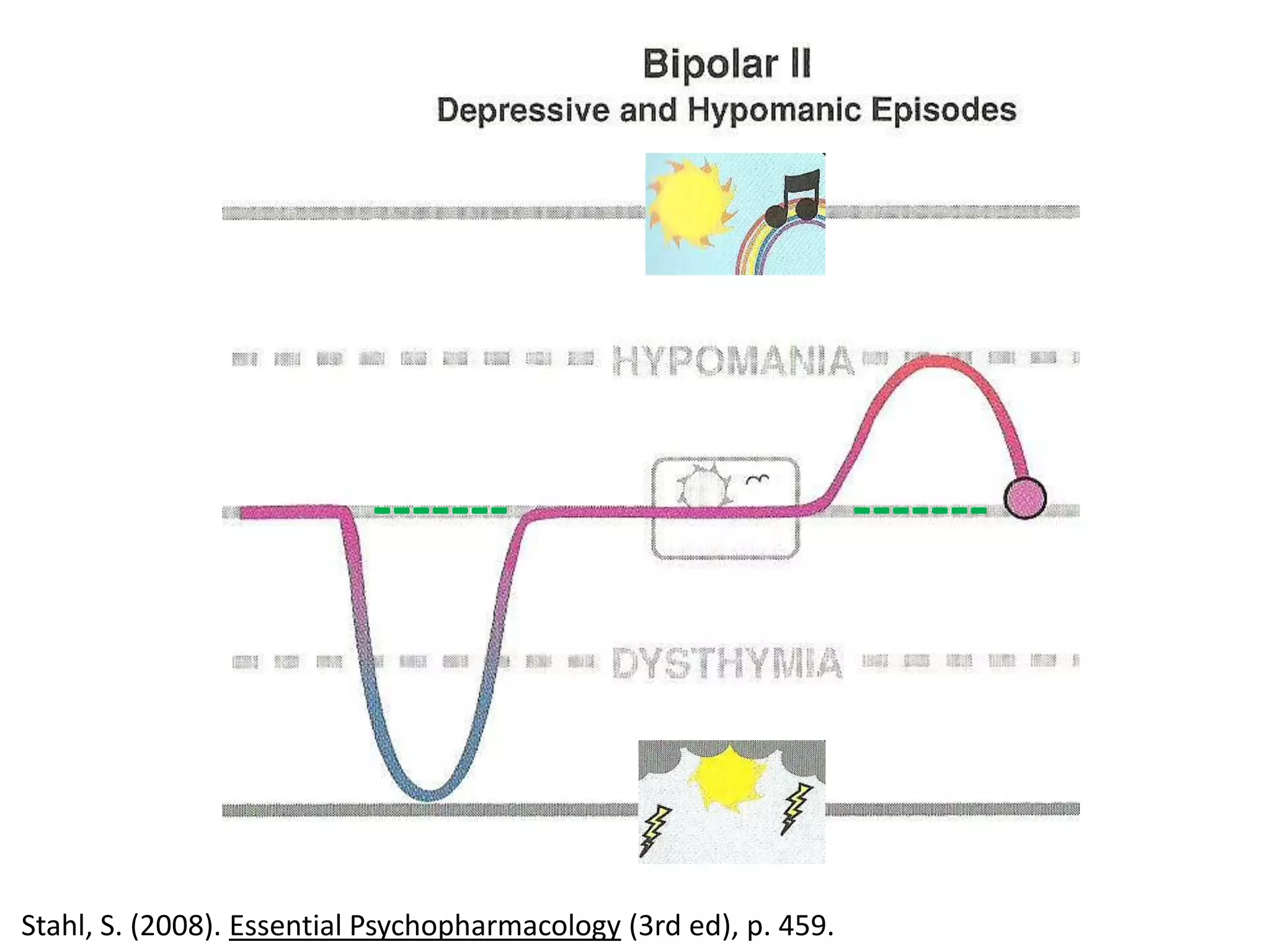
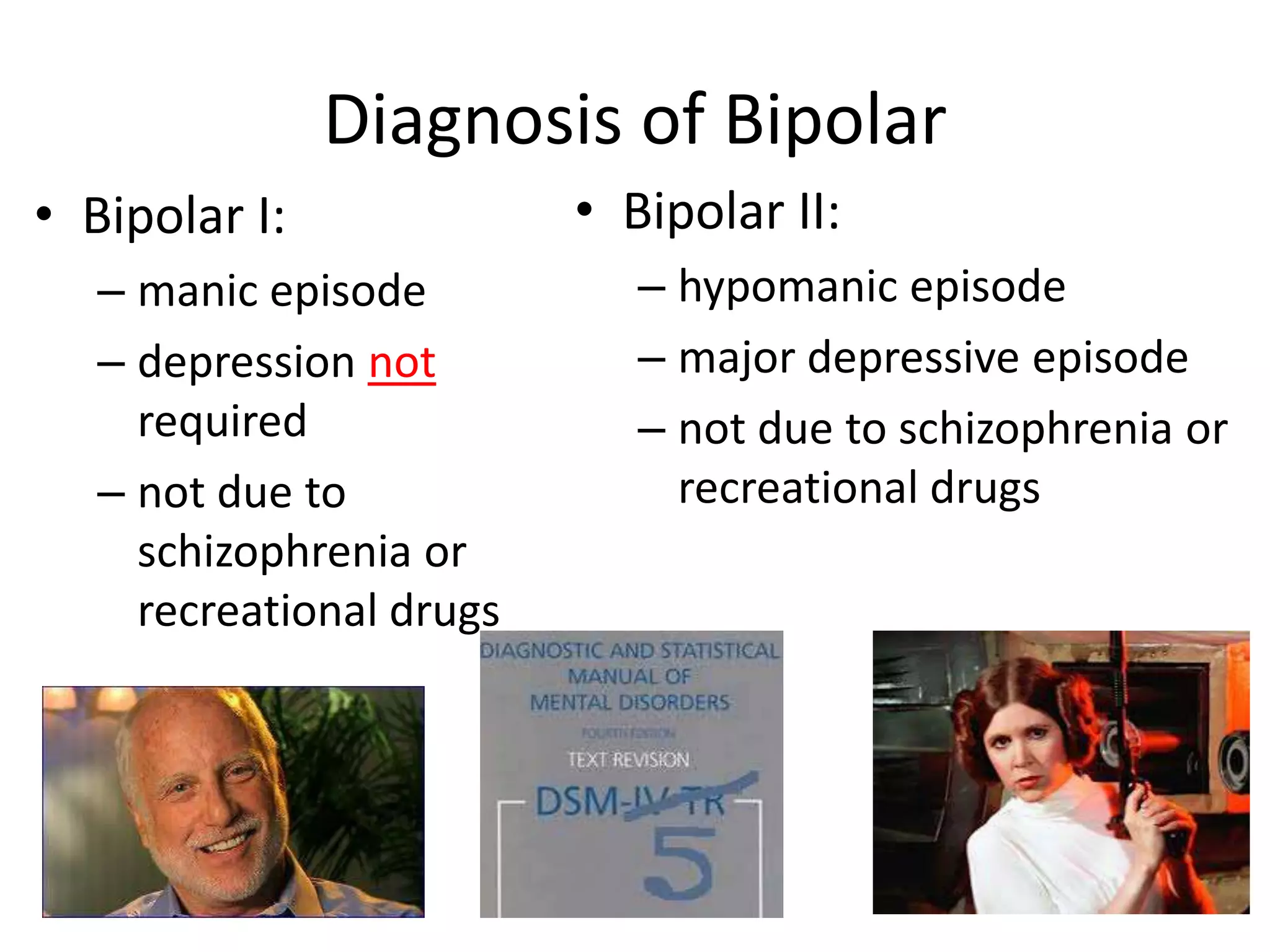
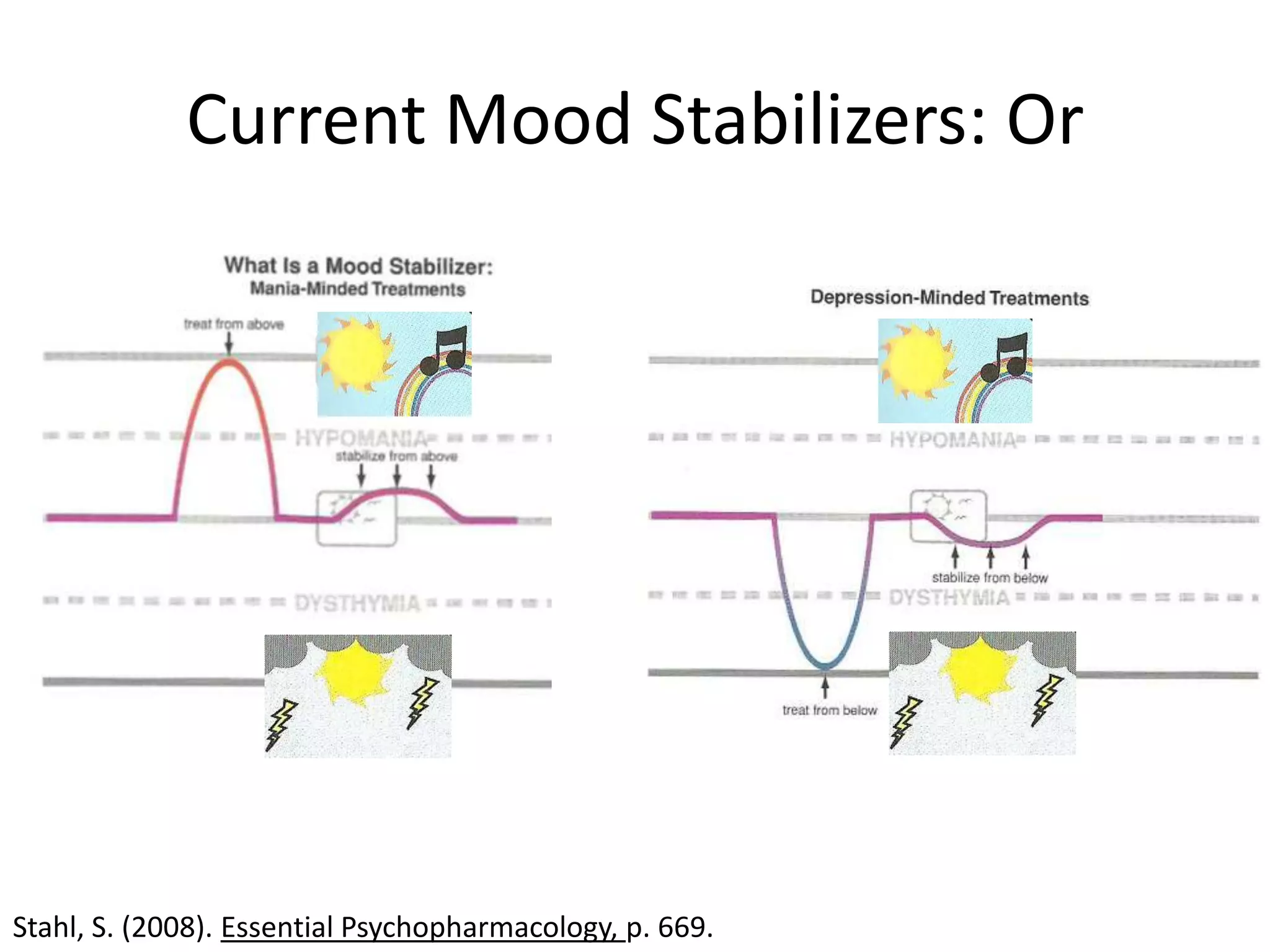
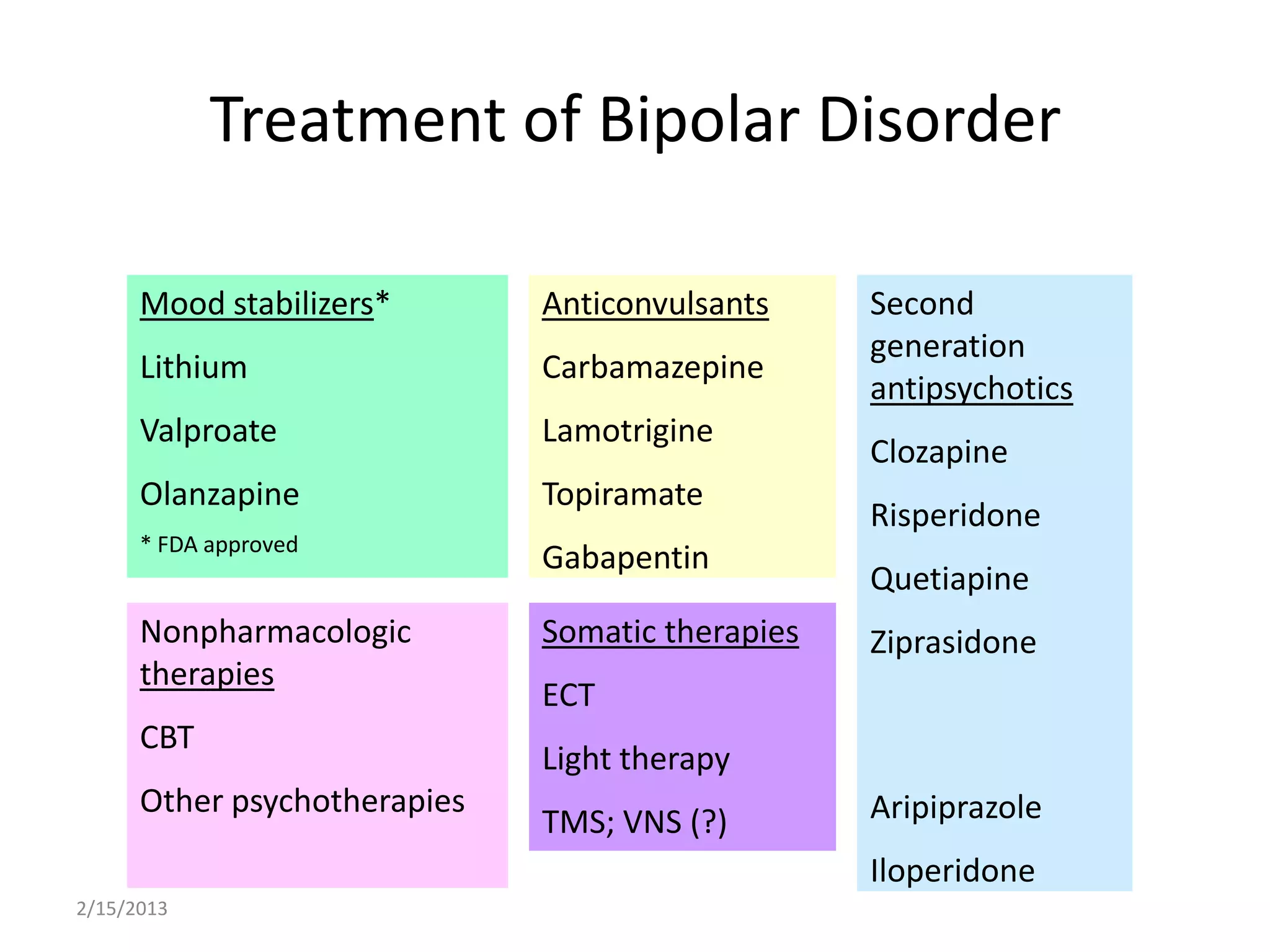
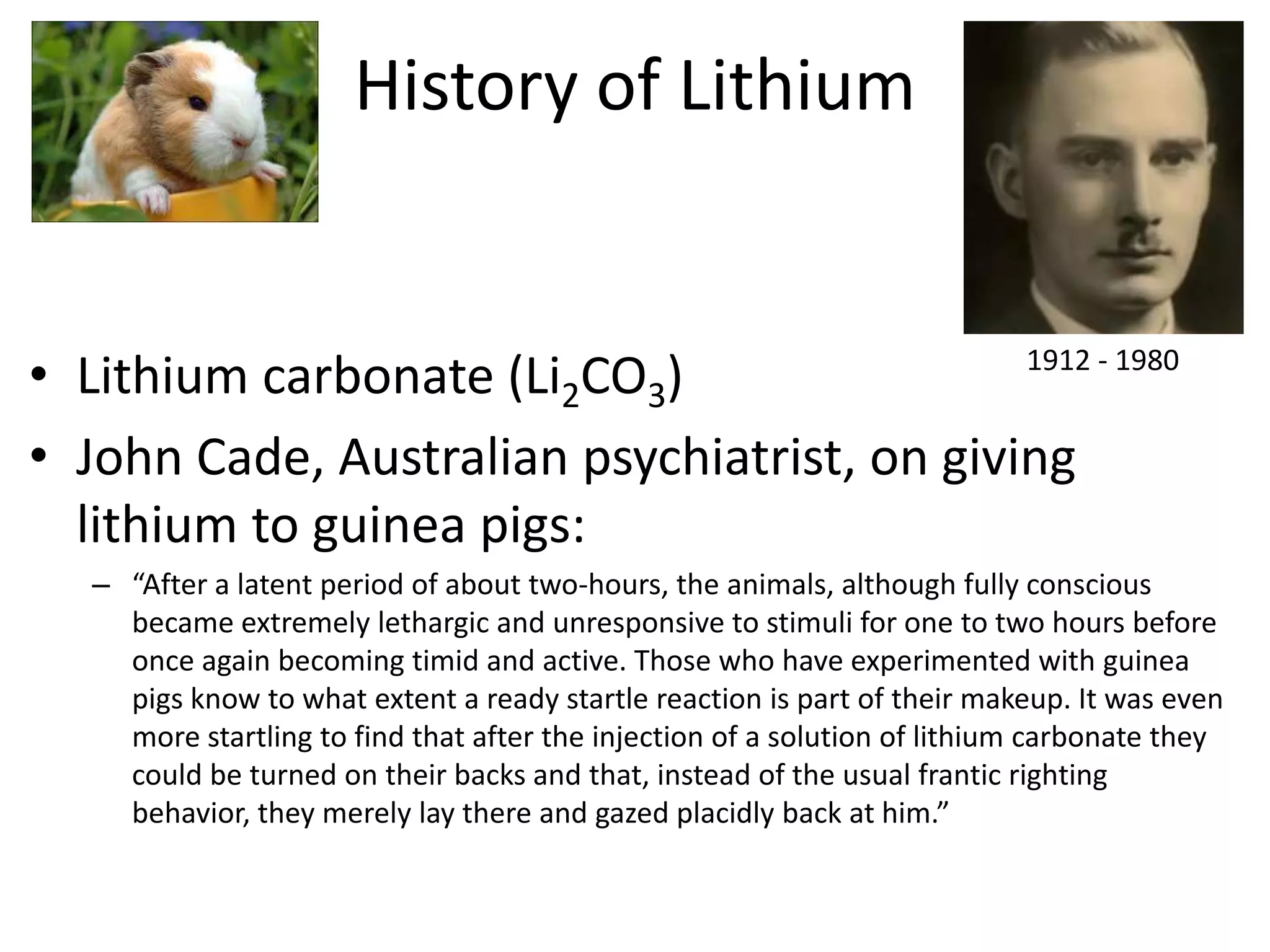
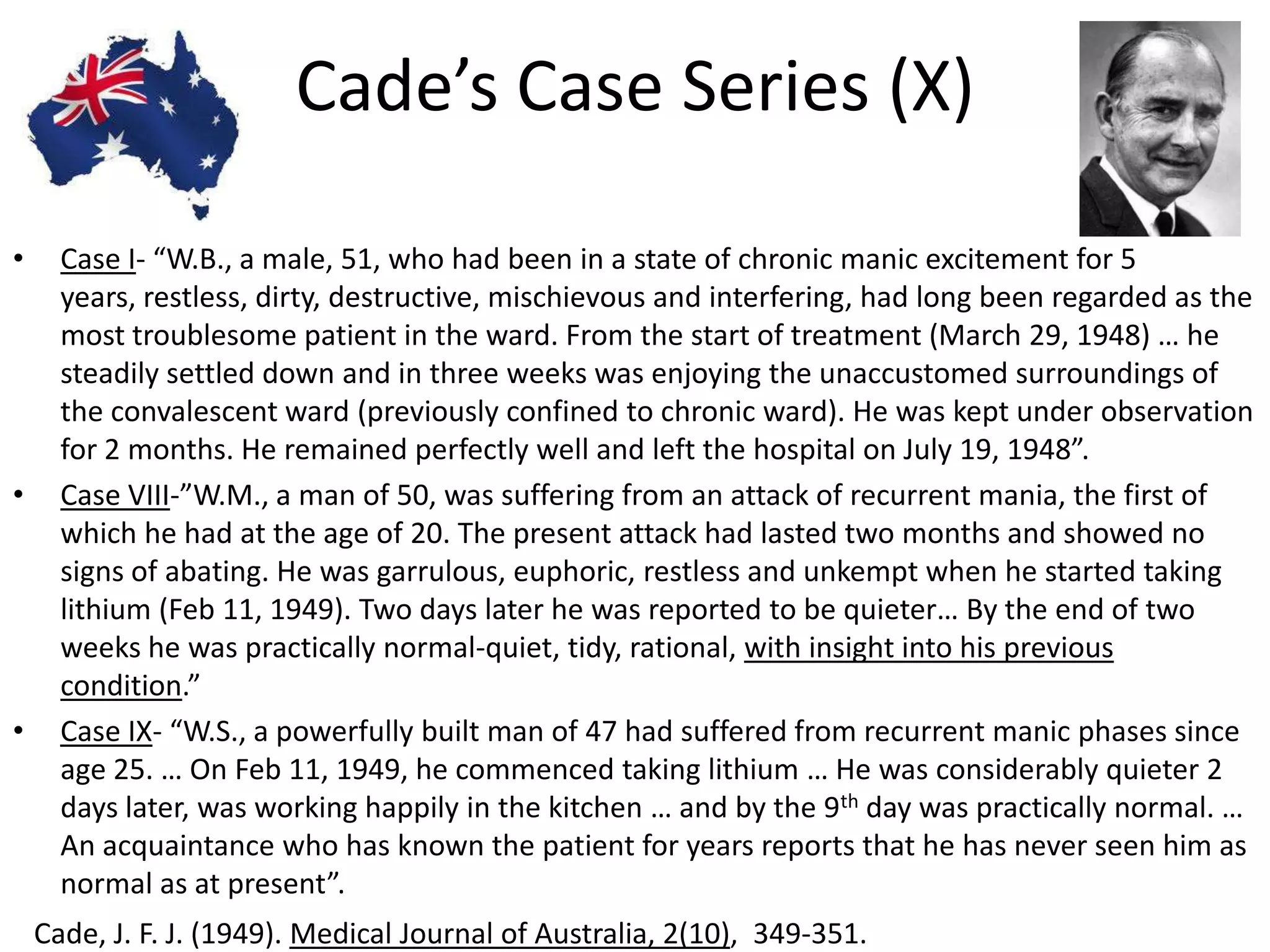
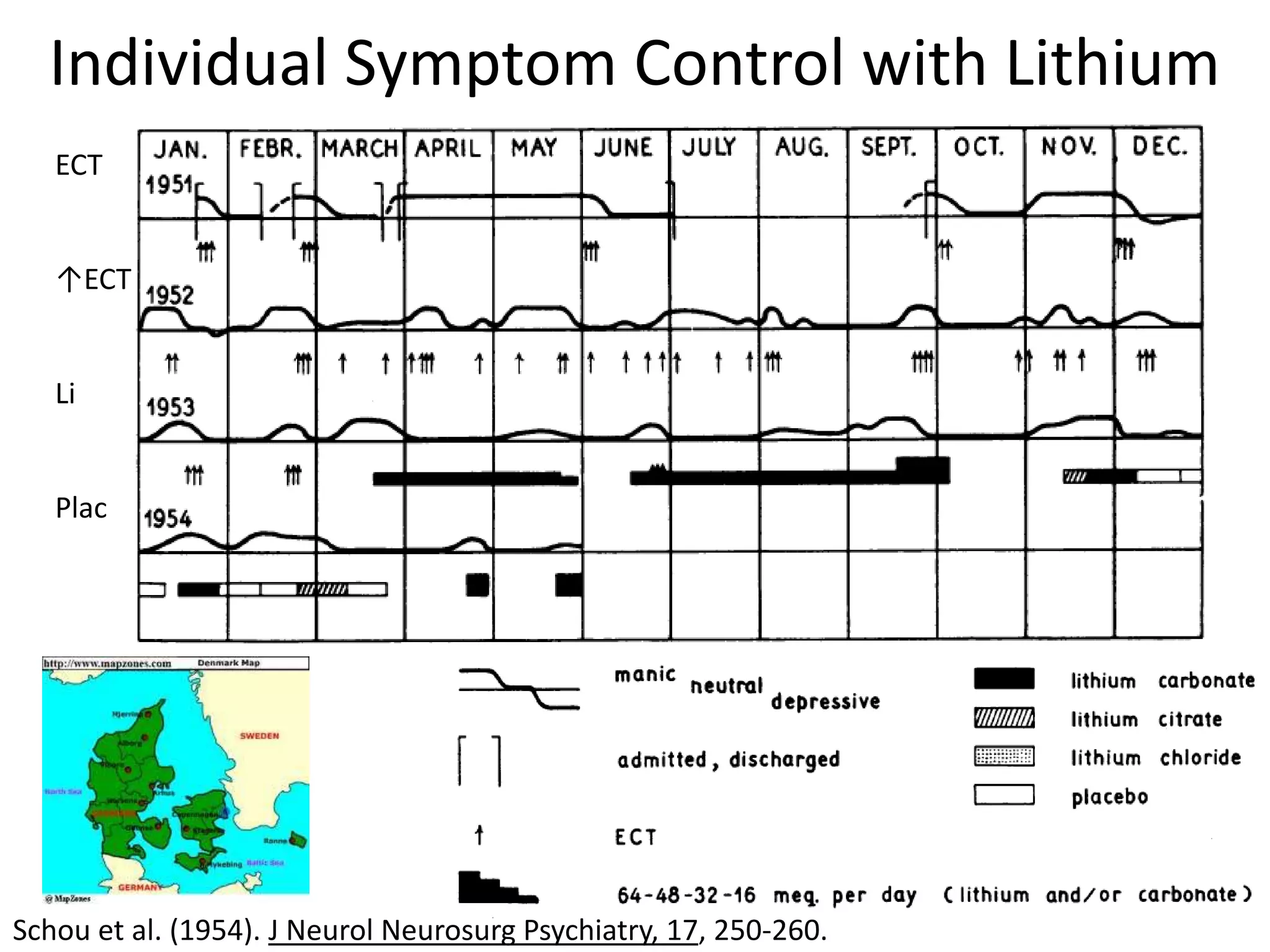
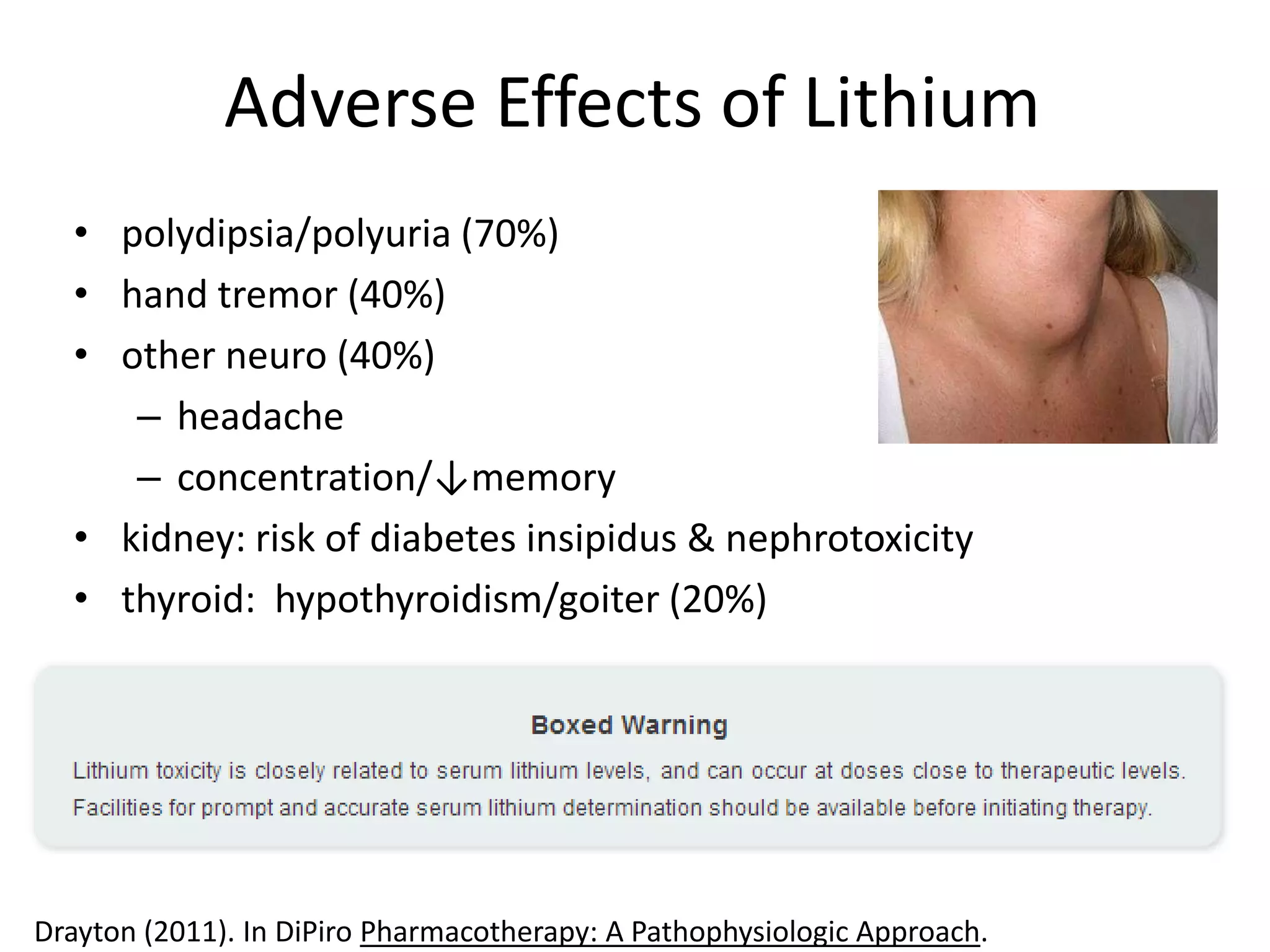
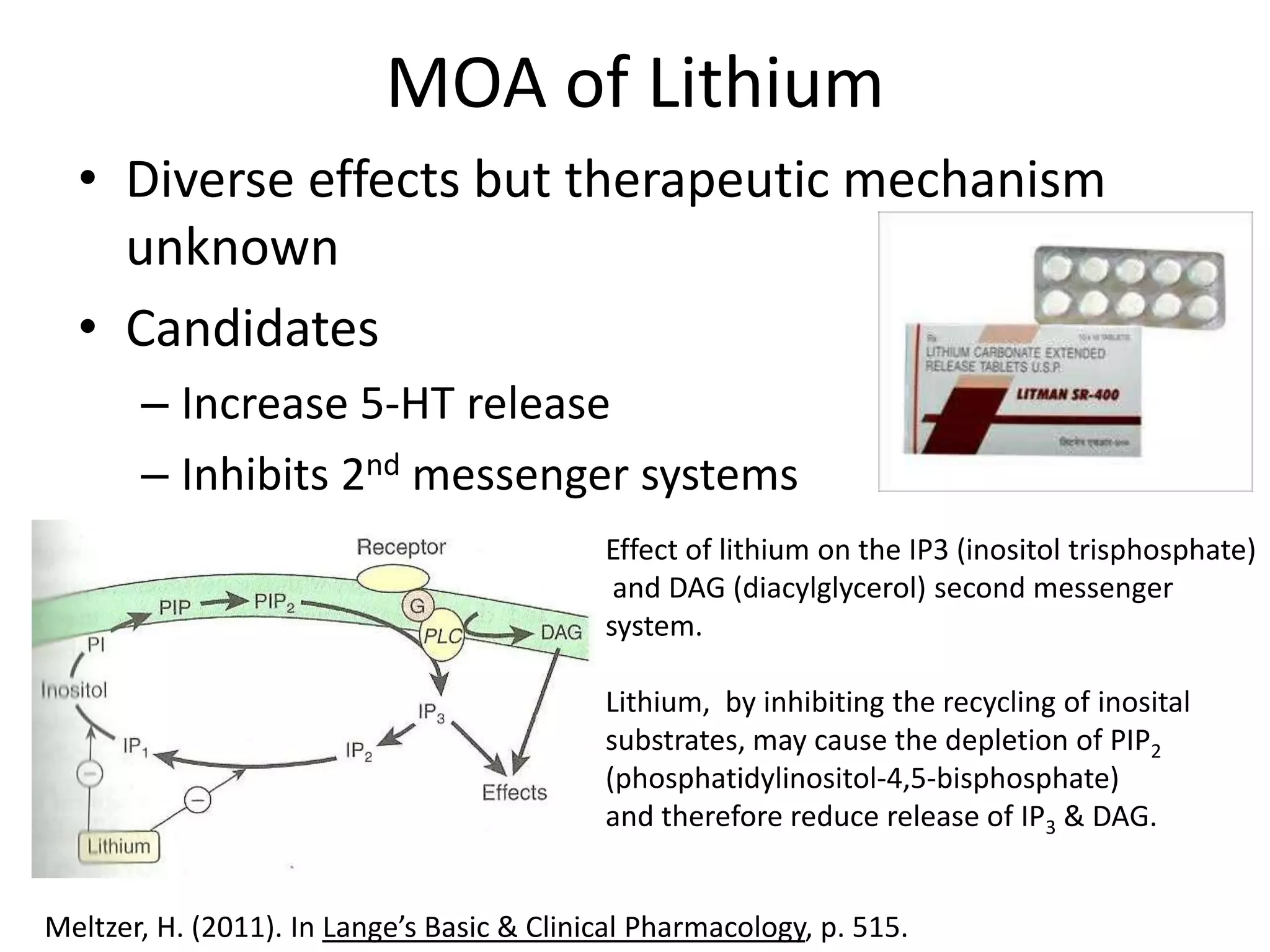
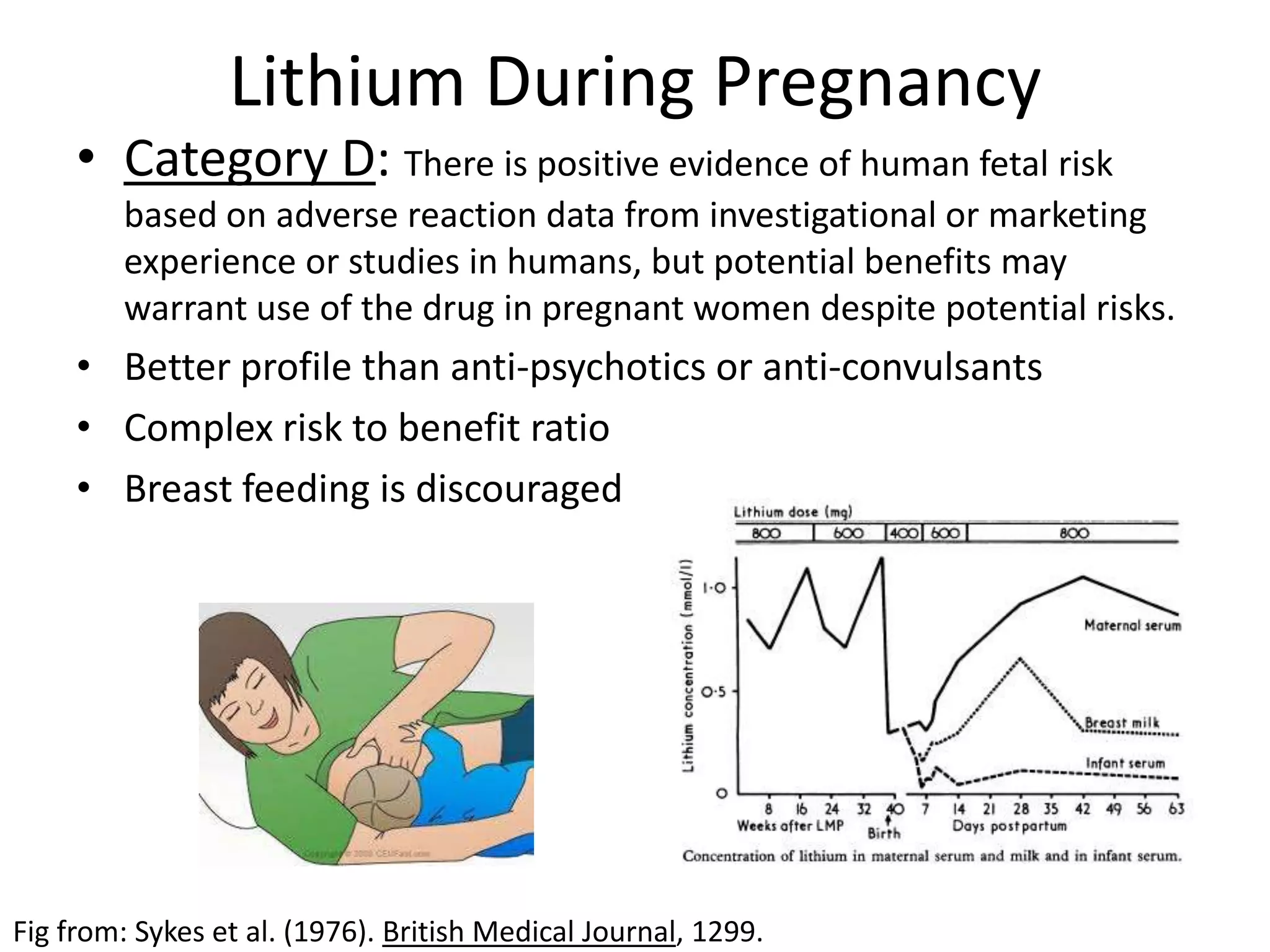
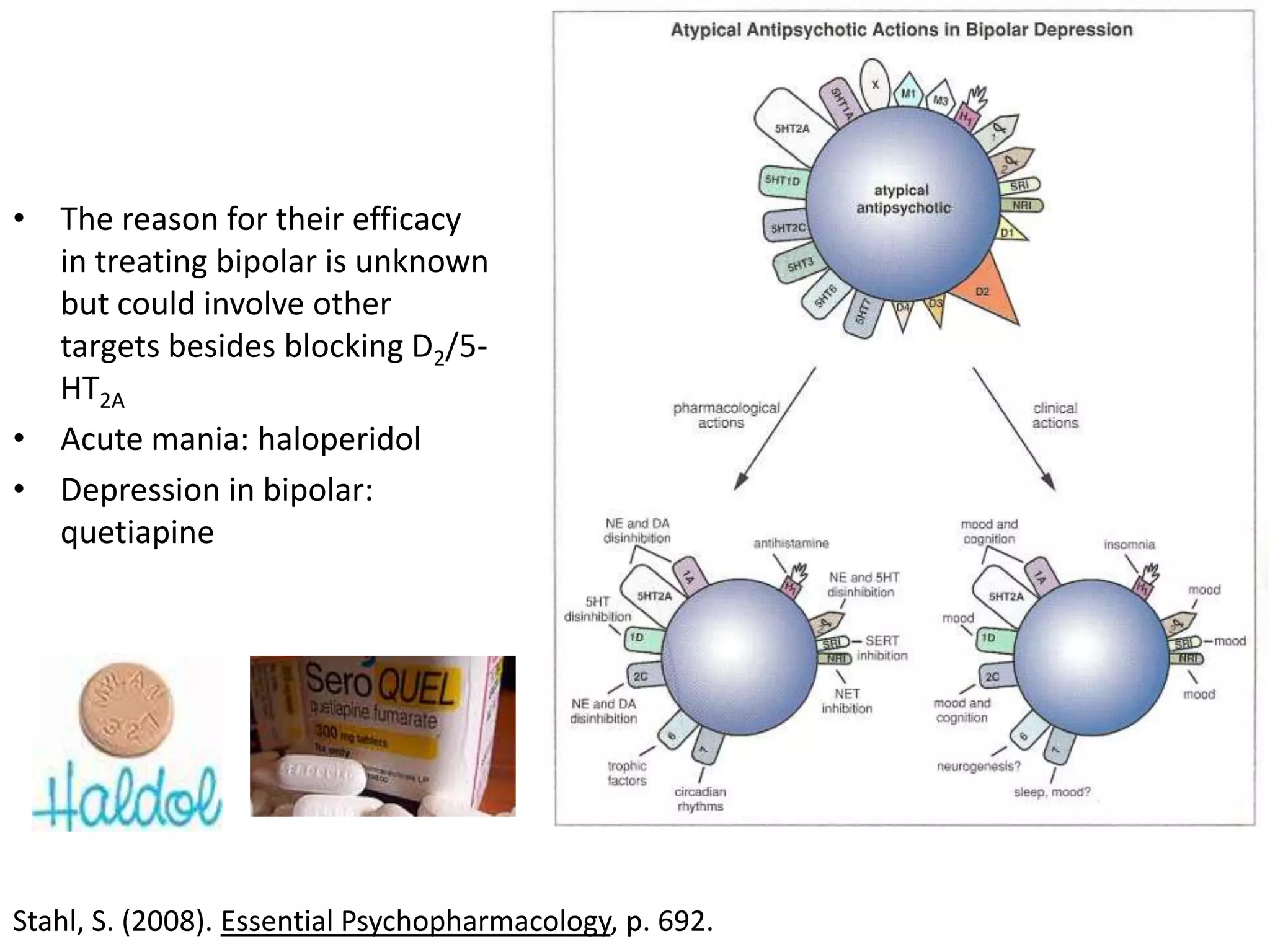

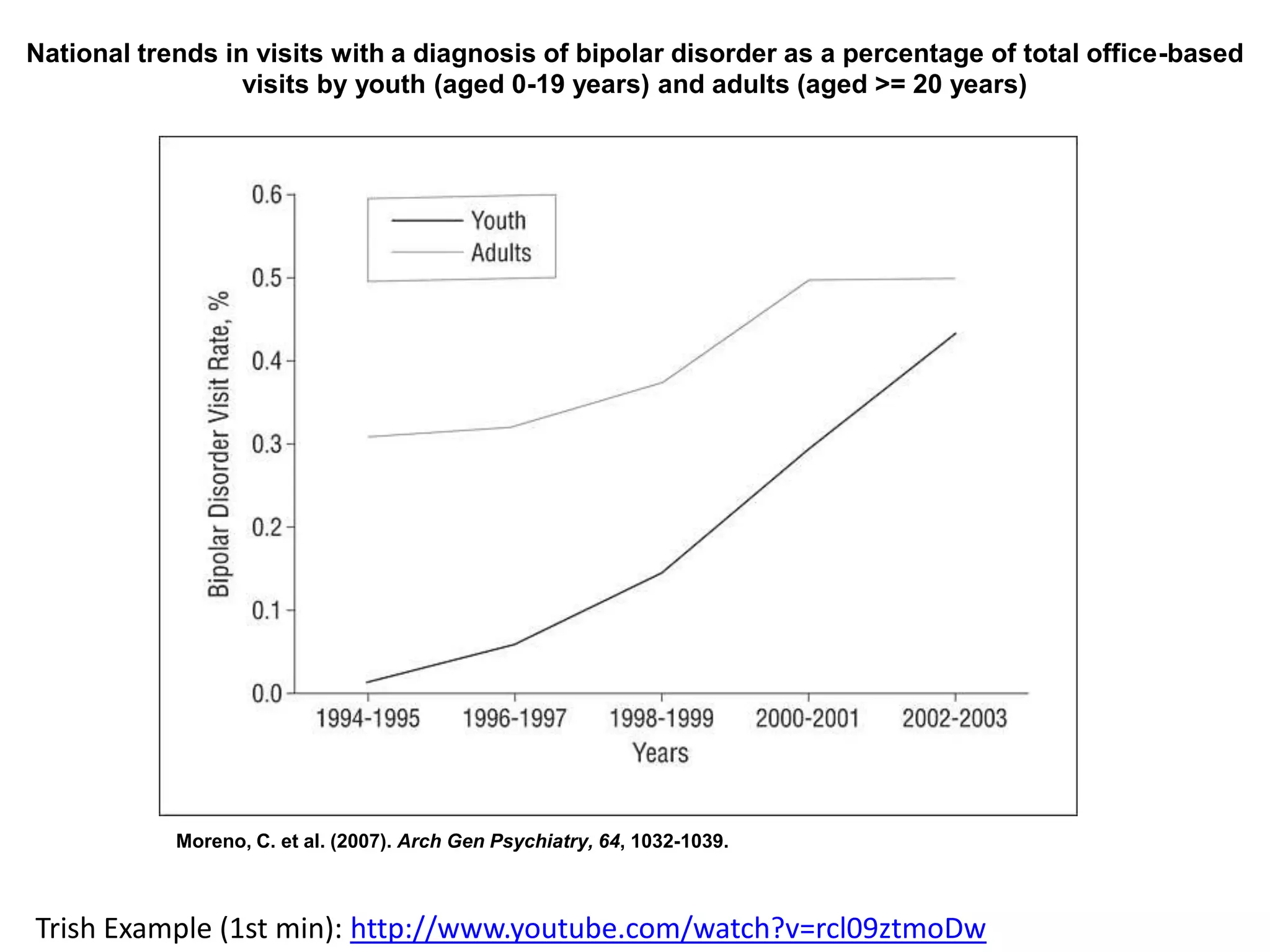

The document discusses bipolar disorder, its subtypes, and the treatment options available, focusing on mood stabilizers such as lithium and anticonvulsants. It outlines the history of lithium, including its initial uses, adverse effects, and its efficacy during pregnancy, while also addressing the importance of drug combinations in treatment despite limited research. Overall, lithium is highlighted as a first-choice treatment for bipolar I disorder, with increasing trends in diagnosing bipolar disorder among youth and adults.























































































