Download as PDF, PPTX


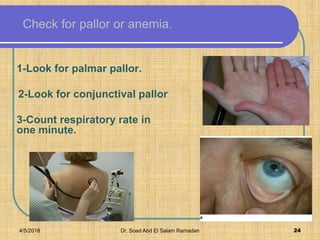


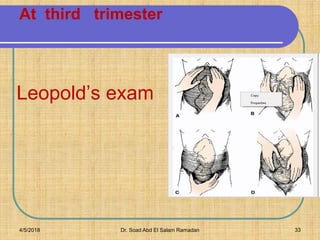



The document discusses antenatal care, which involves comprehensive health supervision of a pregnant woman before delivery. It outlines the goals, objectives, schedule and components of antenatal care visits. Key aspects include taking a detailed medical history, conducting physical examinations including measuring weight, blood pressure and uterine size, and performing routine investigations like urine and hemoglobin tests. Health education is provided on nutrition, exercise, hygiene, medications, infections and potential complications. Supplements like folic acid, iron and calcium are recommended. The document emphasizes monitoring fetal growth and movements, addressing patient concerns at each visit, and preparing for childbirth and potential emergencies.











![Prenatal[2]](https://cdn.slidesharecdn.com/ss_thumbnails/prenatal2-120201201254-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
