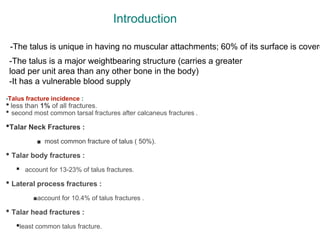
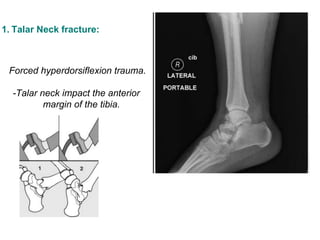
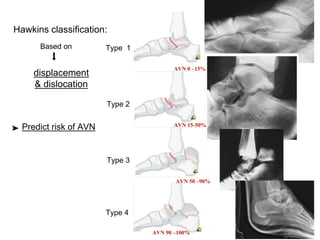
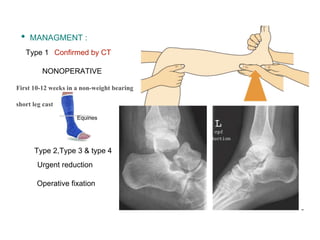
The document discusses various types of talus fractures, including incidence rates, causes, evaluations, and treatment options. It highlights the importance of anatomical reduction and stable internal fixation to minimize complications such as osteonecrosis and posttraumatic arthritis. Fractures of the talus are relatively uncommon but can have serious implications due to the bone's unique anatomy and blood supply issues.