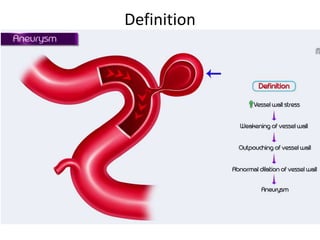
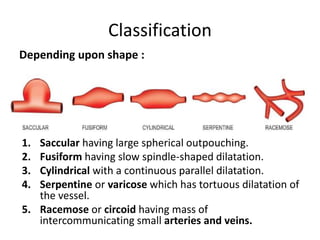
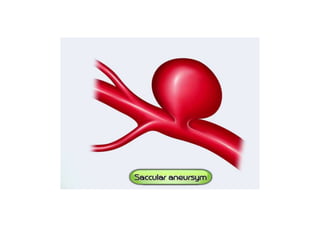
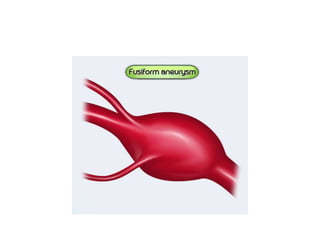
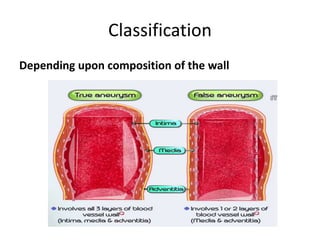
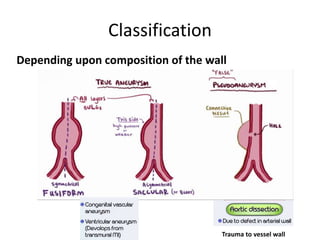
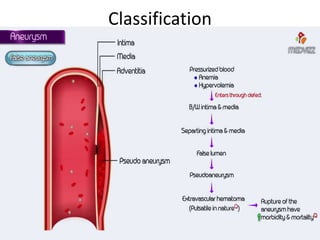
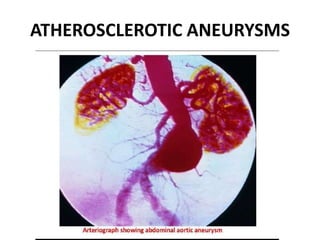
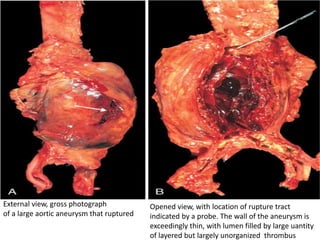
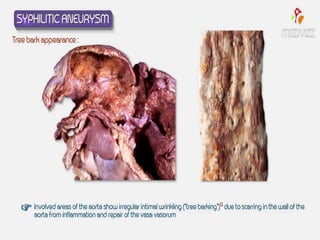
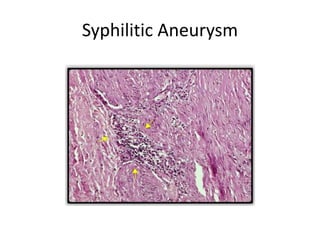
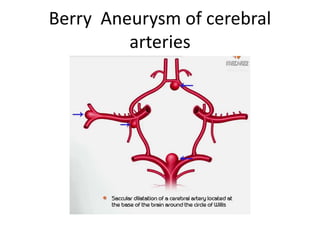
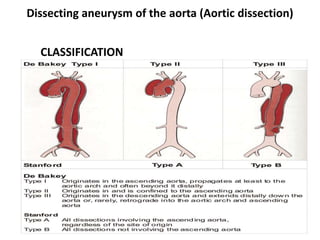
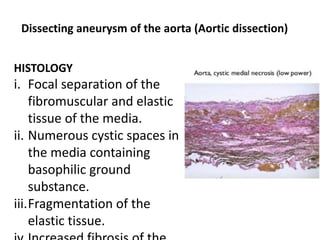
The document discusses aneurysms, detailing their definitions, classifications, pathogenesis, and complications. It categorizes them based on location (arterial and venous), shape (saccular, fusiform, cylindrical, etc.), and composition of the vessel wall, while also exploring various causes including atherosclerosis, infections, and genetic disorders. Additionally, it outlines the pathology of specific types of aneurysms, such as abdominal aortic and syphilitic aneurysms, along with their potential complications.






































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)

















