Mediastinal anatomy
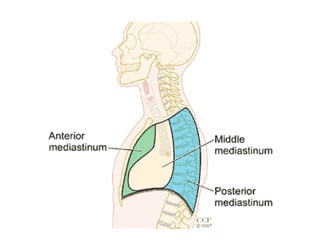
• Themediastinum lies between the right and
left pleurae in and near the median sagittal
plane of the chest.
• It extends from the sternum in front to the
vertebral column behind, and contains all the
thoracic viscera excepting the lungs.
3.
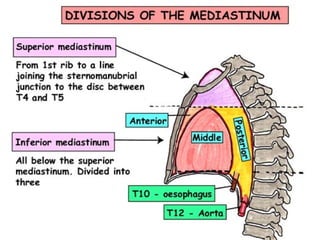
Mediastinal Anatomy
• Includesstructures
bound by:
– the thoracic inlet
– diaphragm
– sternum
– vertebral bodies
– and pleura
• Has 4 compartments
-Superior
-Anterior
-Middle
-Posterior
6.
Mediastinal Anatomy
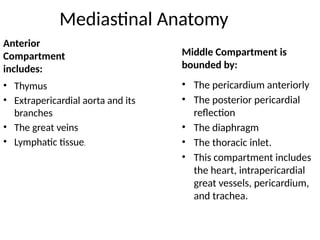
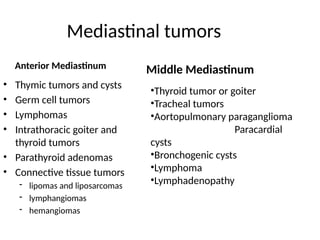
Anterior
Compartment
includes:
• Thymus
•Extrapericardial aorta and its
branches
• The great veins
• Lymphatic tissue.
Middle Compartment is
bounded by:
• The pericardium anteriorly
• The posterior pericardial
reflection
• The diaphragm
• The thoracic inlet.
• This compartment includes
the heart, intrapericardial
great vessels, pericardium,
and trachea.
7.
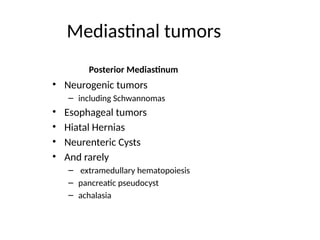
Posterior Compartment:
• Extendsfrom the posterior pericardial
reflection to the posterior border of the vertebral
bodies and from the first rib to the diaphragm.
• Includes the
Esophagus
Vagus nerves
Thoracic duct,
Sympathetic chain, and azygous venous
system.
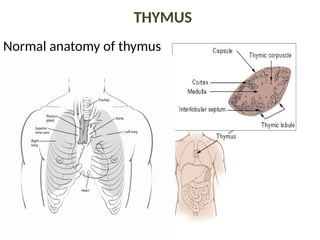
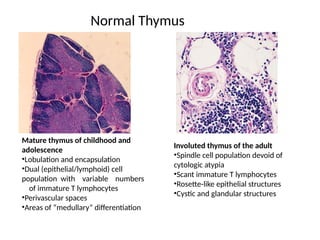
Normal Thymus
Mature thymusof childhood and
adolescence
•Lobulation and encapsulation
•Dual (epithelial/lymphoid) cell
population with variable numbers
of immature T lymphocytes
•Perivascular spaces
•Areas of “medullary” differentiation
Involuted thymus of the adult
•Spindle cell population devoid of
cytologic atypia
•Scant immature T lymphocytes
•Rosette-like epithelial structures
•Cystic and glandular structures
13.
Normal histology ofcortex of thymus
• Histologically, the darkly staining cortex contains
densely packed, small, immature lymphocytes, which
overshadow the sparse epithelial cell population .
• Large, mitotically active lymphoblasts, may be found
in the subcapsular cortex.
• These cells have a round to oval nucleus with one or
two prominent nucleoli and relatively abundant,
strongly basophilic cytoplasm.
• “tingible-body macrophages” can be seen.
14.
Normal histology ofmedulla of thymus
• The medulla is paler staining, less densely
cellular than the cortex.
• Contains more mature T-cells, prominent
epithelial cells , Hassalls corpuscles, admixed
macrophages, dendritic cells , B lymphocytes
and rarely myoid cells.
• The medullary T-lymphocytes are larger, paler-
staining and have more cytoplasm than cortical
lymphocytes.
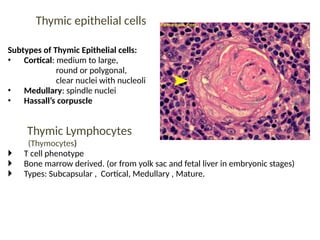
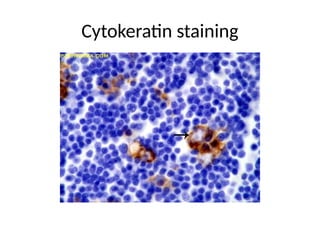
Thymic epithelial cells
Subtypesof Thymic Epithelial cells:
• Cortical: medium to large,
round or polygonal,
clear nuclei with nucleoli
• Medullary: spindle nuclei
• Hassall’s corpuscle
Thymic Lymphocytes
(Thymocytes)
T cell phenotype
Bone marrow derived. (or from yolk sac and fetal liver in embryonic stages)
Types: Subcapsular , Cortical, Medullary , Mature.
17.
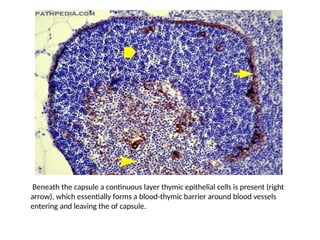
Beneath the capsulea continuous layer thymic epithelial cells is present (right
arrow), which essentially forms a blood-thymic barrier around blood vessels
entering and leaving the of capsule.
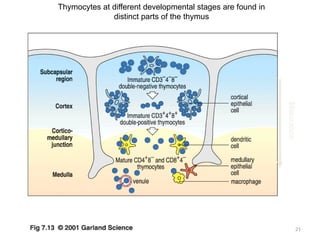
Development of Tcell
• T-cells are continually produced in the bone marrow.
• T-cells in the bone marrow are considered immature
because they are not fully developed. During this
stage, the T-cells do not have receptors on their
surfaces yet because they do not express CD4 or
CD8 glycoproteins (carbohydrate and protein
molecules located on the surface of T-cells).
Therefore, they are considered double-negative
cells (Cd4- Cd8-).
20.
• The cellsthen enter the bloodstream and
travel to the thymus gland, where they
develop into mature T-cells.
• The T-cells develop receptors on their outer
surfaces. This means they express both CD4
and CD8 glycoproteins on their surfaces.
Because they express both glycoproteins,
these cells are called double-positive T-cells
(CD4+ Cd8+).
Dendritic cells
• Aminor cell population in lymphoid tissues,
are specialized for presentation of antigenic
peptides to T lymphocytes.
• Thymic dendritic cells are involved in the
deletion of self-reactive T lymphocytes.
• Developing T cells are negatively selected
predominantly by self antigens presented on
newly formed thymic dendritic cells.
• All dendritic cells are of bone-marrow origin.
23.
• Types ofDendritic cells
1. Myeloid dendritic cells.
• These are most similar to the monocytes.
• The MDC are made up of two subsets.
• The more common mDC-1, which is a major
stimulator of T cells.
• The extremely rare mDC-2, which may have a
function in fighting wound infection.
24.
2. Plasmacytoid dendriticcells
• These look like the plasma cells but have the
certain characteristic of the myeloid dendritic
cells.
• High intracellular MHC II.
• Express CD1a.
• Can produce high amounts of interferon
alpha, so known as IPC (interferon-producing
cells).
25.
Tumours of Thymus
Thethymus contains Corresponding tumour
• Epithelial elements Thymoma
• Lymphoid elements Lymphoma
• Stroma Sarcomas
•Neuroendocrine cells Neuroendocrine
tumours (carcinoids)
• Germ cells Germ cell tumours
26.
Thymoma
Neoplasms of thymicepithelial cells ,
independently of the presence or number of
lymphocytes and without the cytological
atypia of epithelial cells.
• Most common in anterior mediastinum.
• Usually slow growing tumor.
• Yellow-gray with a fleshy lobulated appearance.
• Intraluminal hemorrhage, cystic space, calcification.
• Malignancy determined by tissue invasion > histologic type.
27.
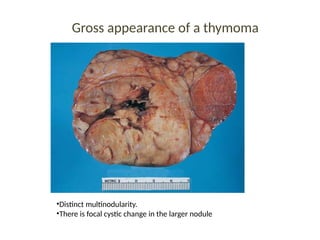
Gross appearance ofa thymoma
•Distinct multinodularity.
•There is focal cystic change in the larger nodule
28.
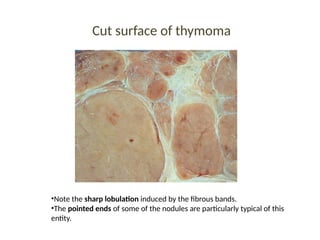
Cut surface ofthymoma
•Note the sharp lobulation induced by the fibrous bands.
•The pointed ends of some of the nodules are particularly typical of this
entity.
Classification of thymoma
Traditionalclassification
• Based on their relative proportion of epithelial cells to lymphocytes
and on the shape of the epithelial cells.
Clinicopathological classification
• Benign
• Invasive
.
31.
Morphofunctional Classification
1) Cortical:similar to those found in the normal cortex.
2) Medullary : predominant epithelial cells with few lymphocytes.
3) Mixed : proliferation of cortical and medullary epithelial cell types
• mixed thymoma of common type
• mixed thymoma with cortical or medullary predominance.
4) Predominantly cortical thymoma (organoid)
5) Well-differentiated thymic carcinoma
32.
The WHO schema(1999)- headed by Juan Rosai
• 3 categories:
A : Nuclei showed a spindle or oval shape
B : Round epithelioid appearance
B1, B2 , B3 on the basis of the proportional
increase (in relation to the lymphocytes) &
emergence of atypia of the neoplastic
epithelial cells.
C : Tumor showing overt cytologic features of
malignancy.
33.
New WHO Classificationof Thymoma (2004)
•Type A
•Type AB
•Type B1
•Type B2
•Type B3
Others
•Micronodular thymoma
•Metaplastic thymoma
•Microscopic thymoma
•Sclerosing thymoma
•Lipofibroadenoma
34.
New WHO classificationof thymoma (2004)
• The most recent version
• Guided by Dr. Muller- Hermelink.
(1) Elimination of the type C thymoma from the
schema, with the latter tumors being segregated
into a separate and distinct category of thymic
carcinoma.
• Reason: All non-organotypic malignant epithelial
neoplasms other than germ cell tumours are
designated thymic carcinomas.
35.
Type A (spindle,medullary) Thymoma
• Neoplastic thymic epithelial cells having
Spindle/oval shape,
Lacking nuclear atypia,
with few or no non-neoplastic lyphocytes.
• Appearance can simulate of a meshenchymal
neoplasm, but IHC shows neoplasm of epithleial
tissue.
• Grossly : well circumscribed and encapsulated.
• C/S :Tan white and shows vague lobulation with
less distinct dissecting white fibrous bands.
36.
Type A (spindle,medullary) Thymoma.
• Microscopically
few or no lymphocytes
Tumor cells are spindle and/or oval shaped with
bland nuclei, dispersed chromatin and
inconspicuous nucleoli.
Arranged in solid sheets without any particular
pattern or in a storiform pattern.
Rosette like formation (without central lumen)
may be present.
37.
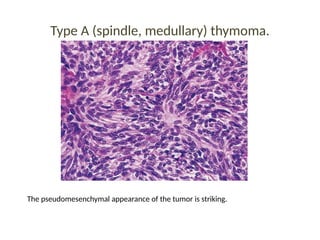
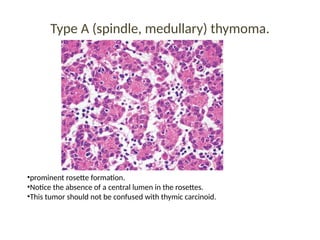
Type A (spindle,medullary) thymoma.
The pseudomesenchymal appearance of the tumor is striking.
38.
Type A (spindle,medullary) thymoma.
•prominent rosette formation.
•Notice the absence of a central lumen in the rosettes.
•This tumor should not be confused with thymic carcinoid.
Type B1 Thymoma
•Lymphocyte-rich thymoma
• Lymphocytic thymoma
• organoid thymoma
• Predominantly cortical thymoma
• Resembles normal functional thymus .
• It is not differentiated from normal thymic cortex with areas
resembling thymic medulla.
• Markers
Keratin
CD1a
CD99
CD3
CD5
41.
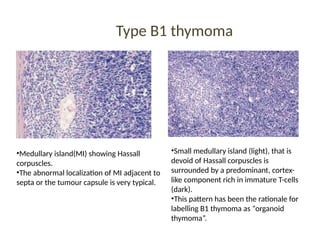
Type B1 thymoma
•Medullaryisland(MI) showing Hassall
corpuscles.
•The abnormal localization of MI adjacent to
septa or the tumour capsule is very typical.
•Small medullary island (light), that is
devoid of Hassall corpuscles is
surrounded by a predominant, cortex-
like component rich in immature T-cells
(dark).
•This pattern has been the rationale for
labelling B1 thymoma as “organoid
thymoma”.
42.
Type B2 (cortical)thymoma
• 18-42% of all thymomas.
• Neoplastic epithelial component appear as scattered plump
cells with vesicular nuclei & distinct nucleoli among heavy
population of lymphocytes.
• Cytoplasm is abundant .Cells are round/polygonal.
“Polygonal cell thymoma”
• Perivascular spaces are common.
• Perivascular arrangement of tumor cells show palisading
effect.
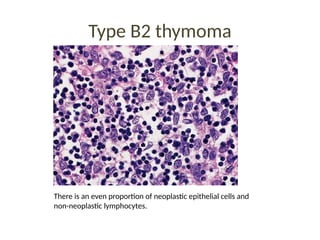
Type B2 thymoma
Thereis an even proportion of neoplastic epithelial cells and
non-neoplastic lymphocytes.
45.
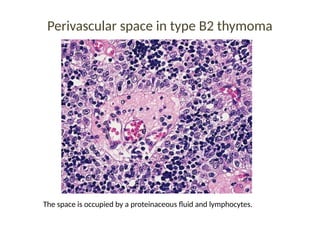
Perivascular space intype B2 thymoma
The space is occupied by a proteinaceous fluid and lymphocytes.
46.
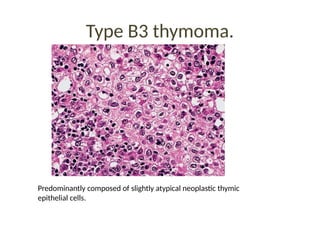
Type B3 thymoma
Well-differentiatedthymic Ca.
Epithelial thymoma
Squamoid thymoma
Atypical thymoma
• Not encapsulated but show a vaguely infiltrative border with
extension into mediastinal fat or adjacent organs.
• Sheet like growth of neoplastic epithelial cells.
• Epithelial cells having round/polygonal shape, no/mild atypia.
• Admixed with minor component of lymphocytes .
• Medullary islands are usually absent
Type AB (mixed)thymoma.
• 15-43% of all thymomas.
• Features of type A thymoma are admixed with
foci rich in lymphocytes.
• Segregation of 2 patterns can be sharp/
indistinct.
50.
Type AB (mixed)thymoma.
The type A areas can be easily confused with hypercellular septa. This is one of
the most common thymoma subtypes.
51.
Thymic carcinoma
• Thymiccarcinoma defined as a thymic
epithelial tumor (i.e., a thymoma) exhibiting
clearcut cytologic features of malignancy.
• The diagnosis is often one of exclusion, in the
presence of a malignant epithelial tumor
located in the thymic region in the absence of
disease in the lung or any other organ.
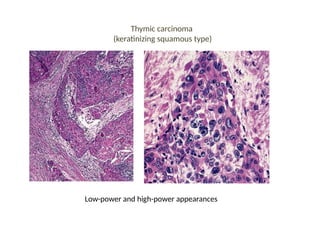
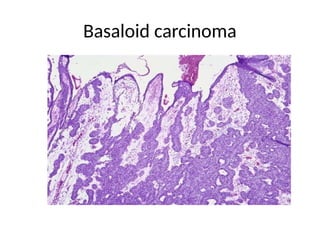
Keratinizing squamous type(thymic
carcinoma)
•This form is rich in atypical epithelial cells, many of
which undergo keratinization.
• The appearance is very similar to that of squamous
cell carcinoma at other sites.
• Microscopically lobular pattern of growth is
generally maintained, and the tumor lobules are
even more widely separated from each other by
fibrous bands than in the other thymoma type.
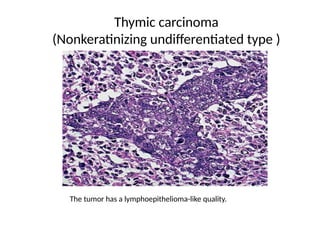
Nonkeratinizing undiffentiated type(thymic
carcinoma)
•Tumor cells are large, deeply acidophilic nucleoli that are
sharply outlined and perfectly round are one of the
hallmarks of this neoplasm, which is also characterized by a
‘syncytial’ appearance.
• The lymphocytes of this tumor, which can be very
numerous, have the phenotype of mature peripheral T cells
rather than the immature thymocytic phenotype seen in
ordinary thymoma.
• It becomes undiffentiated from, that of so-called
‘lymphoepithelioma’ of the tonsil and nasopharynx.
• The tumor cells are consistently immunoreactive for keratin.
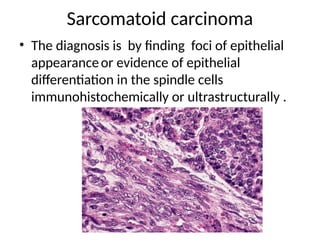
Sarcomatoid carcinoma
• Thediagnosis is by finding foci of epithelial
appearanceor evidence of epithelial
differentiation in the spindle cells
immunohistochemically or ultrastructurally .
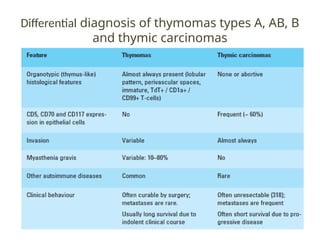
Proposed Terminology by
Susterand Moran
Tumors displaying most or all of the organotypical features of
thymic differentiation and absence of cytologic atypia are classified
as well-differentiated thymic epithelial neoplasms (ie, thymoma);
Tumors that retain only some of the organotypical features of
differentiation of the thymus but that already display mild to
moderate cytologic atypia are classified as moderately
differentiated thymic epithelial neoplasms (ie, atypical thymoma);
Tumors characterized by total absence of the organotypical features
of the thymus and showing overt cytologic evidence of malignancy
correspond to poorly differentiated thymic epithelial neoplasms
(ie, thymic carcinoma)
63.
Prognosis
Stage :single most important factor.
Microscopic Type: Increasing aggressiveness .
A<AB<B1<B2<B3<C
Presence of invasion : important prognostic factor
Completeness of excision.: important
Myasthenia gravis: good prognostic factor: earlier
detection, benefits of steroids.
64.
Poor prognostic factor
•Invasion into the surrounding fat,pleura,pericardium.
• Intrathoracic or extrathoracic metastases.
• Tumor size > 10cm , age < 30 yreas.
• Tracheal or vascular compromise.
• Epithelial and mixed histologies.
• The presence of hematologic paraneoplastic
syndrome.
65.
Points To BeRemember…….
• Thymoma is Neoplasms of thymic epithelial cells.
• Associated with Myasthenia gravis (30-45%)
• WHO Classification System Correlates with clinical
aggressiveness ,likelihood of invasion,prognosis,Risk, therapeutic
decisions .
• New WHO Scheme: type C thymoma is eliminated & segregated into
a separate and distinct category of thymic carcinoma.
• All thymic epithelial neoplasms should be regarded as malignant
neoplasms.
• Presence of invasion & Completeness of excision are important
prognostic factor.
• Thymectomy is Primary treatment.
Carcinoid tumors
• Itis a malignant neoplasm that invades locally
and metastasizes distantly.
• Thymic carcinoid usually lacks endocrine
manifestations but sometime associated with
cushing syndrome and carcinoid tumor of
other sites, such as bronchus or ileum.
• Multiple endocrine neoplasia (MEN) type 1
or2a.
68.
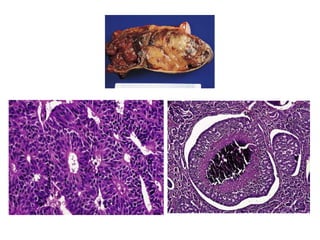
• Grossly,
Solid,
Well circumscribed but not encapsulated
Lacks the distinct lobulations of thymoma .
It may be highly vascularized and frankly
hemorrhagic.
• Microscopically,
Ribbon and festoon formation, rosette-like glands
with central lumina.
‘Balls’ of cells with central necrosis and calcification, marked
vascularization.
The tumor cells have a more granular cytoplasm than those
of thymoma, the nuclear chromatin is slightly coarser, and
mitotic activity is frequent.
Frequent lymphatic and blood vessel invasion.
70.
Immunohistochemically
• keratin, chromogranin,synaptophysin, neuron-
specific enolase, and other general endocrine
markers.
Morphologic variants
• Spindle cell pattern
• Prominent oncocytic component
• With melanin pigment
71.
Small cell neuroendocrinecarcinoma
• It is indistinguishable from that of its pulmonary
counterpart.
• Thymic tumors have a mixture of small cell
neuroendocrine carcinoma and squamous cell
carcinoma,and sometime combining features of
carcinoid tumor and small cell carcinoma in the
same lesion.
• The tumor cells are elongated, with darkly staining
nuclei and scanty cytoplasm with extensive necrosis
Large cell neuroendocrine carcinoma
• seen exeptionaly.
72.
Tumor like lesion
Thymiccyst
Divided into two distinct types.
• Unilocular thymic cysts
• Multilocular thymic cyst
73.
Unilocular thymic cysts
•Developmental origin.
• Arise from remnants of the third branchial
pouch-derived thymopharyngeal duct.
• They are generally small, and located in the neck
more often than in the mediastinum.
• The wall is thin and translucent, and inflammation
is usually lacking.
• The epithelial lining is flattened, cuboidal,
columnar, or (rarely) squamous.
• Thymic tissue is present in the wall, some of it
connecting with the lining epithelium.
74.
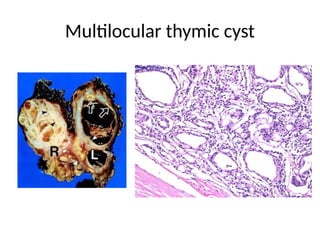
Multilocular thymic cyst
•Is in an acquired process of a reactive nature.
• It is always accompanied by inflammation and fibrosis.
• The lining of the individual cysts may be flat, cuboidal,
ciliated columnar, or (often) squamous, either single or
stratified .
• Some areas have highly reactive appearance,
occasionally acquiring the features of
pseudoepitheliomatous hyperplasia.
• Cholesterol granulomas are common.
• In some instances the inflammatory infiltrate is very
prominent, with formation of numerous lymphoid
follicles.
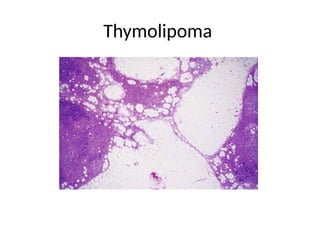
Stromal tumors
Thymolipoma
• Encapsulatedbenign thymic lesion that can attain a
huge size and can simulate radiographically
cardiomegaly or pulmonary sequestration.
• Microscopically, there is an admixture in various
proportions of mature adipose tissue and
unremarkable thymic tissue.
Variants
• An abundance of fibroconnective tissue
thymofibrolipomas.
• An abundance vessels thymohemangiolipoma
Thymic stromal sarcomas
•low-grade malignant mesenchymal tumors.
• Their microscopic appearance is variable, but
well-differentiated liposarcoma/atypical
lipomatous tumor is the predominant
component (‘thymoliposarcoma’).
• Others stromal tumors are
osteosarcoma ( arising in an ectopic
hamartomatous organ)
kaposiform hemangioendothelioma in an
infant.
THYROID AND PARATHYROIDLESIONS
• Mediastinal thyroid tumors are usually large
goiters that are continuous with the thyroid gland
in the neck.
• They are treated by excision, usually using a
median sternotomy.
• The most common pathologic change in
mediastinal thyroid glands is nodular hyperplasia.
81.
• Thyroid nodularhyperplasia in the
mediastinum may occur in the form of
independent nodules ( parasitic or accessory
nodules).
• The nodular hyperplasia arise from cervical
thyroid that has been pulled down either into
the anterior prevascular compartment or the
retrotracheal compartment (‘posterior
descending goiter’) .
82.
• Gross images:mediastinal
thyroid gland with nodular hyperplasia show
s anatomically separate nodules (AFIP)
• Microscopically: normal appearing thyroid
tissue with colloid-filled or hyperplastic
follicles; similar findings in thyroid gland.
83.
Parathyroid tumors
• 7%of parathyroid adenomas are found in the
superior mediastinum. Others are located in
the anterior mediastinum .
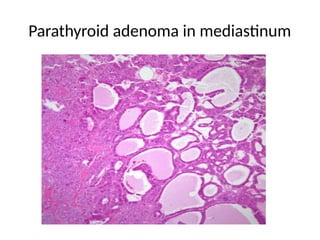
• Parathyroid adenoma in the mediastinum
showing oncocytic features and a
pseudoangiomatoid growth pattern admixed
with solid areas.
Mediastinal parathyroid carcinomas
• Have also been reported, some of them being
nonfunctioning.
GERM CELL TUMORS
•Germ cell tumors includes approximately 20%
of the mediastinal tumors and cysts.
• Primary origin from extragonadal germ cells.
• Possibility of any mediastinal germ cell tumor
representing a metastasis from a testicular or
ovarian primary lesion should always be
investigated.
• Associated with the klinefelter syndrome.
86.
Seminoma OR Germinoma
•Seminoma of the mediastinum arises almost
always within the thymus .
• The morphologic appearance is identical to
that of its testicular counterpart at the light
microscopic, immunohistochemical, and
ultrastructural level.
• They are different in their KRAS sequence and
p53 immunostain profile.
87.
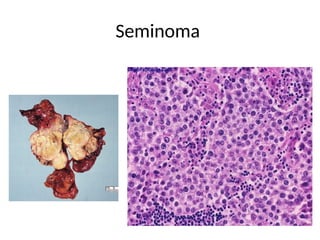
Grossly
• solid
• homogeneous
•no necrosis.
Microscopically,
• Compact nests of large tumor cells
• Lage amount of cytoplasmic gycogen and irregular ,skein
like nucleolus, surrounded by fibrous septa which is
infiltrated by lymphocytes and plasma cells.
• Epithelioid granulomas, numerous germinal centers.
Diffential diagnosis
Thymoma
Large cell lymphoma
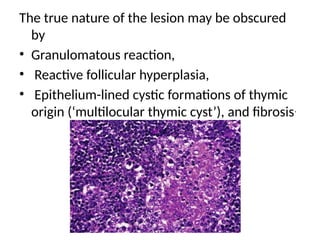
The true natureof the lesion may be obscured
by
• Granulomatous reaction,
• Reactive follicular hyperplasia,
• Epithelium-lined cystic formations of thymic
origin (‘multilocular thymic cyst’), and fibrosis.
90.
• Seminomas areimmunoreactive for placental
alkaline phosphatase (PLAP), OCT4, SALL4,
M2A, AP-2 gamma, CD117, and often CD57
(Leu7).
• The primary treatment is with radiation
therapy, and the prognosis is very good.
91.
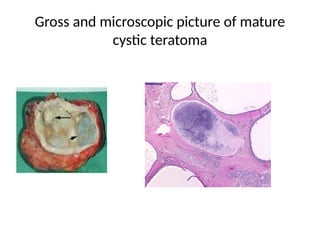
Mature Cystic Teratoma
•Mature cystic teratoma is the most common type
of mediastinal germ cell neoplasm.
• It usually occurs in early adult life.
• Grossly
large size and has a
distinct, sharply delineated wall that often becomes
calcified.
The cut surface is predominantly cystic and
adherence to surrounding structures is common.
92.
• Microscopicaly
resembles thatof the more common mature
cystic teratoma of ovary.
The cysts are lined by stratified squamous
epithelium and contain sebaceous glands and
hair follicles.
Other common components are neural tissue,
gastrointestinal tract, cartilage, and
respiratory structure,
islet cell elements.
Complications
Prominent xanthogranulomatous
inflammation ifthe sebaceous material within
it escapesse.
Perforation into the tracheobronchial tree .
Dense adhesions often found in this tumor
may be the result of pancreatic enzyme
secretion.
• Prognosis of mature teratoma is excellent.
95.
Immature teratoma
• Asa germ cell tumor similar to mature
teratoma but also containing immature
epithelial, mesenchymal, or neural elements
without a component of embryonal
carcinoma.
• Numbers of cases in mediastinam is too less.
96.
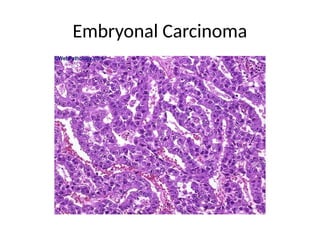
Embryonal Carcinoma
• Itis an invasive, highly necrotic neoplasm.
• Microscopically
Poorly differentiated.
The tumour cells form sheets, tubules or papillae.
The cells are large and polygonal or columnar with large
vesicular nuclei having one or more prominent nucleoli.
The cytoplasm is variably basophilic, eosinophilic or clear.
There is a high mitotic rate, with atypical mitoses.
Necrosis is particularly common in combined yolk sac
tumours.
• Immunohistochemically, there is reactivity for keratin,
PLAP, CD30, and CD57 .
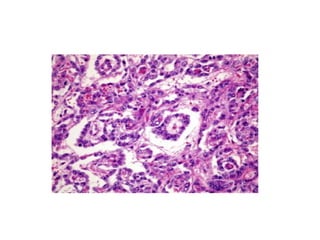
Yolk sec tumors
•Endodermal sac tumor,
• It may occur admixed with other germ cell elements
or (more rarely) as a pure neoplasm.
• Yolk sac elements are more common in mediastinal
than in testicular neoplasm.
• Microscopically
Multiple communicating channels,
Penivascular mantles of cells resembling immature
glomeruli(Shiller-Duval bodies).
Intra- and extracellular hyaline globules all arranged
in a loose reticular network .
100.
• Mediastinal yolksac tumors may have
prominent spindle cell features ,contain a
hepatoid component or be accompanied by
secondary multilocular cystic changes in the
adjacent non-neoplastic thymus.
• The prognosis of pure endodermal sinus
tumor is very poor.
101.
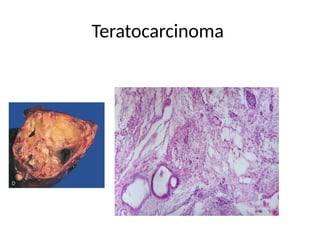
Teratocarcinoma
• It isdefined as the combination of embryonal
carcinoma and teratoma (mature and/or immature).
• It Comprises about 5% of all mediastinal germ cell
tumors.
• It grows rapidly and infiltrates widely.
• Grossly,
areas of hemorrhage and necrosis are present.
• Microscopically,
Areas of embryonal carcinoma alternate with
mature foci, with an abundance of foci of
intermediate differentiation.
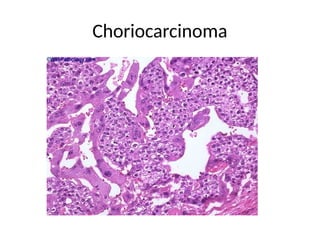
Choriocarcinoma
• It occursin the third decade of life.
• It is associated with gynecomastia and by elevated serum
levels of human chorionic gonadotropin (hCG).
• Grossly,
large, soft, extensively hemorrhagic, and with foci of necrosis.
• Microscopically
Dual cell population composed of cytotrophoblastic cells with
uniform, round nuclei, clear cytoplasm, and prominent
nucleoli admixed with large, multinucleated
syncytiotrophoblastic cells with bizarre nuclei, prominent
nucleoli, and abundant eosinophilic cytoplasm.
• The prognosis is extremely poor
MALINGNENT LYMPHOMA
• Malignantlymphoma can present as an anterior,
superior, or middle mediastinal mass, in this
order of frequency.
• The majority of malignant lymphomas presenting
as primary mediastinal neoplasms fall into one of
the four categories .
Hodgkin lymphoma
Lymphoblastic lymphoma
Large cell lymphoma
Marginal zone B-cell lymphoma
106.
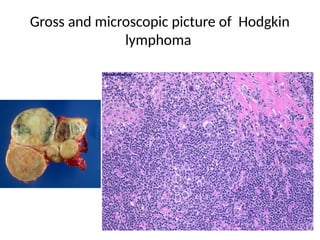
Hodgkin lymphoma
• MediastinalHodgkin lymphoma can involve
primarily the thymus or the lymph nodes or
both sites.
• Most patients are young adults, and more
case seen in females.
• The disease present with local pressure
symptoms (dyspnea, cough, chest pain)..
107.
• Primary Hodgkinlymphoma always of the
classic type, nodular sclerosis subtype.
• Grossly
Sharply outlined
Surrounded by a thick capsule.
The nodules may be multiple and residual
thymic tissue is usually identified.
The consistency is hard, and the cut surface is
vaguely or distinctly nodular .
108.
• cyclin E,CD79a and BOB.1, may be helpful in
the differential diagnosis of cHL and PMBCL.
109.
Microscopicaly
The low-power appearancemay resemble that
of true thymoma by the presence of cellular
nodules encircled by fibrous bands.
Polymorphic, with lymphocytes, plasma cells,
eosinophils, histiocytes, Reed–Sternberg cells
and the their mononuclear variants, and
lacunar cells which provide the diagnosis.
Sometime associated with epithelial-lined
cysts, Hassall corpuscles, and isolated thymic
epithelial cells.
• Diffential diagnosis
Granulomatous’thymoma
Non-Hodgkin lymphoma
Germ cell tumor
Sclerosing mediastinitis
Castleman disease.
Thymic carcinoma
• The disease can spreads subdiaphragmatically
in the absence of supraclavicular lymph node
involvement.
• The primary treatment is usually combination
chemotherapy and radiotherapy.
112.
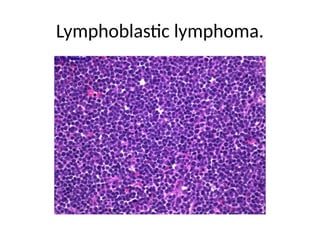
Lymphoblastic lymphoma
• Lymphoblasticlymphoma occurs primarily in the
thymic region.
• It is usually of immature T-cell type ( precursor T
lymphoblastic lymphoma in the WHO
classification). Some cases have been found to be
of pre-T-cell type and natural killer cell type.
• Males are more commonly affected .
• The disease is usually restricted to the
supradiaphragmatic region, with frequent
involvement of cervical, supraclavicular, and
axillary nodes.
113.
Grossly
Solid, softand,nonencapsulated .
Some preservation of the thymic shape can be
appreciated in early cases.
Microscopically
Thymic parenchyma infiltrat by
lymphocytes ,lymphocytes are atypical, with a
very fine chromatin pattern, frequent nuclear
convolutions ( convoluted cell lymphoma),
Numerous mitotic figures, and equally
numerous necrotic cells. .
114.
Fibrosis and formationof multilocular thymic
cysts .
Sometime scattering of eosinophils, and focal
granulomatous reaction can be seen.
• There is usually extension into the perithymic fat,
and invasion of blood vessel walls is frequent .
Diffential diagnosis
• Acute lymphoblastic leukemia
• Thymoma
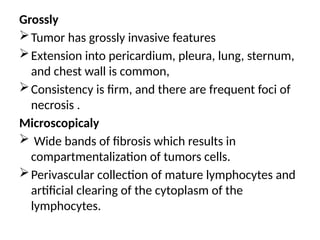
Large cell lymphoma
•Mediastinal large cell lymphoma can present
as a mass in the thymus with or without
lymph node involvement.
• Most patients are young adult females, and
presentation with superior vena caval
syndrome .
117.
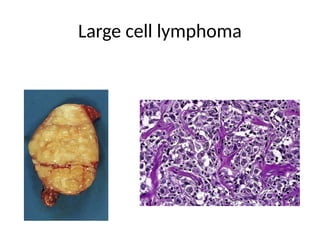
Grossly
Tumor has grosslyinvasive features
Extension into pericardium, pleura, lung, sternum,
and chest wall is common,
Consistency is firm, and there are frequent foci of
necrosis .
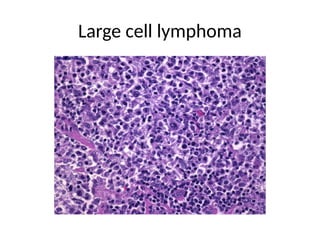
Microscopicaly
Wide bands of fibrosis which results in
compartmentalization of tumors cells.
Perivascular collection of mature lymphocytes and
artificial clearing of the cytoplasm of the
lymphocytes.
• Immunohistochemical reactivityfor CD45
CD30,CD23,CD10,BCL6.
• Diffential diagnosis
Epithelial, germ cell, or neuroendocrine
neoplasm
Thymoma
Seminoma
Larg cell malignent lymphoma
• Tumor can recurs within the chest and spreads
to other sites, including peripheral lymph nodes
and central nervous system.
• An excellent response to radiation therapy and
chemotherapy
121.
Marginal zone B-celllymphoma
• Most commonly occur in female.
• It is associated with Sjögren disease or rheumatoid
arthritis,lymph node or gastric involvement.
Microscopicaliy
Tumors are predominantly composed of small
lymphocytes with a variable admixture of
monocytoid cells and plasma cells.
• Immunohistochemically -Cytokeratin , CD20 , CD3 ,
CD23 , CD43 , CD5 .
122.
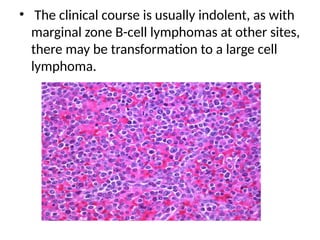
• The clinicalcourse is usually indolent, as with
marginal zone B-cell lymphomas at other sites,
there may be transformation to a large cell
lymphoma.
NEUROJENIC TUMORS
• Neurogenictumors mostly occurs in the
posterior mediastinal.
• It can occurs in both adult and children.
Two main catagories
Tumors of sympathetic nervous system
Tumors of peripharal nerve sheeth
125.
Tumors of sympatheticnervous system
• This occurring in patients younger than the
age of 10 .
• Radiographicaly most tumors of the
sympathetic nervous system have an
elongated tapered appearance.
126.
Neuroblastomas
• Occurs inpatient younger than 1 year.
• The main difference between the mediastinal
and retroperitoneal tumors is the greater
degree of differentiation seen in the former.
• Grossly
large and encapsulated.
Cut section is lobulated architecture and a soft
to fleshy consistency.
Hemorrhage.
127.
• Microscopically
Proliferation ofsmall, round blue cells with
hyperchromatic nuclei, “salt and pepper” chromatin, and
indistinct cytoplasm.
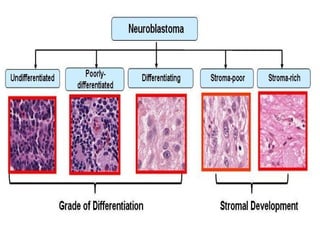
• Divided into differentiating, poorly differentiated, and
undifferentiated subtypes.
• Differentiating tumors have ganglionic differentiation
of 5% to 50% of neoplastic cells
• Poorly differentiated tumors have <5% ganglionic
differentiation
• Undifferentiated tumors have no ganglionic
differentiation and lack fibrillary network of neuropil.
129.
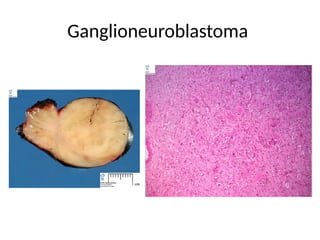
Ganglioneuroblastoma
Intermediate degree ofdifferentiation and that is
related to differentiating neuroblastoma and immature
ganglioneuroma .
• Grossly
Better circumscribed than neuroblastoma .
Surrounded by a well-formed capsule.
• Some of these cases have been associated with
inappropriate secretion of antidiuretic hormone.
• Microscopically
Both mature gangliocytes and immature neuroblasts
and has intermediate malignant potential.
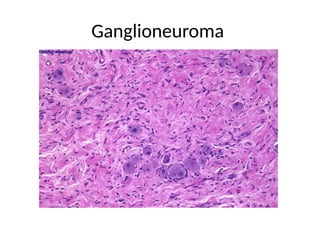
Ganglioneuroma
• It occursin older children and in adults and is
the most common of the three tumors.
• Grossly,
Well-encapsulated mass.
The consistency is soft, and the cut surface is
yellowish gray,
It may contain cystic areas and fatty
degeneration, but fresh necrosis is generally
absent .
Microscopically,
Admixture ofmature ganglion cells and
spindle cells, which could be a Schwann cells
or satellite cells
The ganglion cells may have several nuclei
and are often arranged in clusters.
Focal collections of lymphocytes.
• These tumors can be multiple and can occur
in different locations, with various degrees of
differentiation.
• Prognosis oftumors of the sympathetic
nervous system is directly related to the
degree of differentiation of the tumor.
• The prognosis in neuroblastoma is the least
favorable for the entire group.
• Relapses in the central nervous system have
occurred in some cases of intrathoracic
neuroblastoma.
136.
Tumors of peripheralnerves
The three major tumors in this category are
• Shwannoma
• Neurofibroma
• Malignant peripheral nerve sheath tumor
(MPNST)
137.
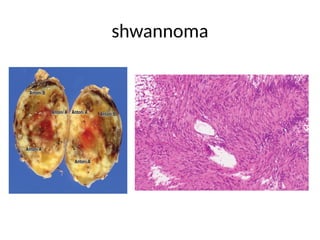
Shwannoma (neurilemoma)
Grossly.
Truly encapsulatedneoplasms of the human
body and is almost always solitary .
Larger schwannomas often contain cystic
area.
Microscopic
Two different patterns usually can be
recognized, designated by Antoni as A and B.
The type A areas are quite cellular, composed
of spindle cells often arranged in a palisading
fashion or in an organoid arrangement
(Verocay bodies)
• Some schwannomascan be very cellular,
somewhat pleomorphic, and mitotically
active, and thus be confused with sarcoma.
140.
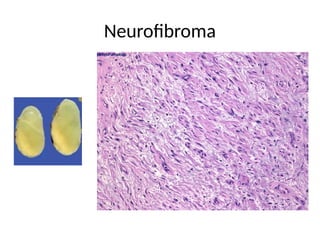
Neurofibroma
• Grossly
Surrounded bya complete fibrous capsule.
• Microscopically
Proliferation of all the elements of a peripheral nerve:
axons, Schwann cells, fibroblasts, and perineural cells.
Schwann cells usually represent the predominant
cellular element.
Most have markedly elongated nuclei, with a wavy,
serpentine configuration and pointed ends .
• Neurofibroma inmost other locations is a
nonencapsulated tumor, because of the large
size that it can reach at this site.
• Therefore the presence of encapsulation
cannot be used as a distinguishing feature
between the two types of benign peripheral
nerve tumor.
143.
• Most benignperipheral nerve sheath tumors
are asymptomatic and are discovered
incidentally on chest x-ray examinations
• The prognosis for both schwannoma
(including its cellular variant) and
neurofibroma is excellent, excision being
curative .
144.
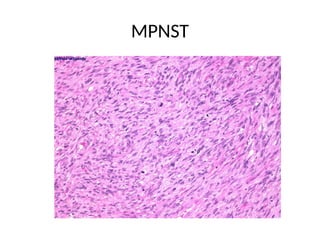
MPNST(malignant peripheral nervecell tumor)
• MPNST of mediastinum may arise de novo or, more
commonly, in the setting of neurofibromatosis type 1
• Microscopically
Dense cellular fascicles which alternate with myxoid
regions.
This swirling arrangement of intermixed dense and
myxoid areas has been described as a marbleized
pattern .
The cells may be spindle shaped with very irregular
contours. Alternatively, cells may be rounded or
fusiform in shape .
Nuclear palisading has also been shown but in less
than 10% of cases and even then, only focally.
145.
• In malignantchange, the tumor cells become
bizarre, and it may then be impossible to
recognize the malignant tumor as originating
from a preexisting neurofibroma.
• Some mediastinal MPNSTs have areas of
glandular differentiation or rhabdomyoblastic
features (so-called ‘triton tumor’).
• The prognosis is generally poor, seems to be
related to resection status, tumor size, and
tumor grade.
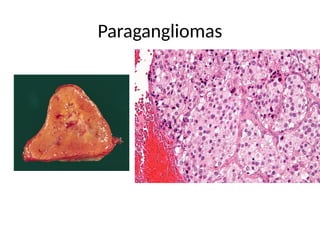
TUMORS OF PARAGANGLIA
•Mediastinal paragangliomas, originate from
the supra-aortic or aorticopulmonary bodies
and are therefore found in the anterosuperior
portion of the mediastinum, in the area of the
aortic arch.
• Others arise from aorticosympathetic
paraganglia and are located in the
costovertebral sulcus. .
149.
• Grossly
Sharply circumscribedpolypoid masses
Firm to rubbery consistency.
Highly vascular tumors and may have a deep red
color.
• Microscopically
Tumor cells are readily recognized
Individual tumor cells are polygonal to oval and are
arranged in distinctive cell balls, called Zellballen.
These cell balls are separated by fibrovascular
stroma and surrounded by sustentacular cells.
MESENCHYMAL TUMORS
Lipoma
• lipomais one of the most common benign
mesenchymal neoplasms of the mediastinum.
• It is very large and located just above the
diaphragm,sometime it extends into both pleural
cavities.
• Diffential diagnosis includes
thymolipoma,lipometosis,cushing disease,or steroid
therapy.
• Other benign adipose tissue tumors of the
mediastinum include lipoblastoma and
lipoblastomatosis of infancy, hibernoma, angiolipoma,
and angiomyolipoma.
152.
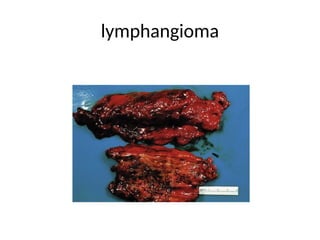
Lymphangioma is anothercommon mediastinal
neoplasm .
• Seen in the anterosuperior mediastinum of
children and in continuity with a cervical
components.
• Lymphangioma has circumscribed patter of
growth.
• Lymphangiomyoma and
lymphangiomyomatosis occur exclusively in
females.
• anastomosing lymphaticspaces.
• Numerous lymphocytes and a few red blood
cells are present in the lymphatic channels.
Moderate amount of fibrous stroma is present
in the walls.
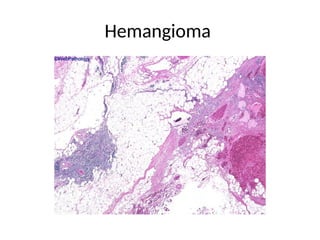
• Hemangioma inadults is usually of the
cavernous variety .
• Microscopically, it is composed of dilated
vessels lined by attenuated endothelium,
separated by fine septa. Foci of thrombosis,
calcification, and cholesterol granulomas may
be present.
• Other vascular tumors are Glomus tumors,
Hemangiopericytomas, epithelioid
hemangioendothelioma and Angiosarcoma .
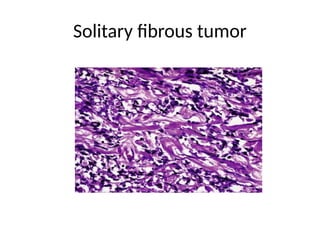
• Solitary fibroustumor of the mediastinum is
the mediastinal equivalent of solitary fibrous
tumor of the pleura.
• Most originate from the mediastinal
(including thymic) stroma.
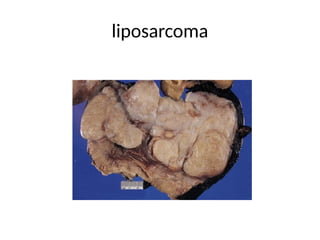
Liposarcoma predominates amongthe
malignant mesenchymal neoplasms
• Sometime associated with liposarcoma of
thigh or retroperitoneum as a manifestation of
multicentric disease.
• Most mediastinal liposarcomas are well-
differentiated tumors.
Others rare tumorsare
• Rhabdomyoma
• Leiomyoma
• Synovial sarcoma
• low grade fibromyxoid sarcoma,
• Leiomyosarcoma
• chondrosarcoma
• Rhabdomyosarcoma
• Alveolar soft part sarcoma giant cell tumor of
soft parts
• Malignant mesenchymoma, and so-called
malignant fibrous histiocytoma.
163.
METASTATIC TUMORS
• Sometumors metastatic to the mediastinum
can mimic clinically and radiographically a
primary mediastinal neoplasm.
• Most common example are undifferentiated
carcinoma of the lung.
• Appearing as a huge mediastinal mass in the
presence of a small, radiographically
undetectable bronchial lesion.
164.
• Direct mediastinalextension can also occur
with tumors of the
esophagus, pleura, chest wall, vertebra, or
trachea.
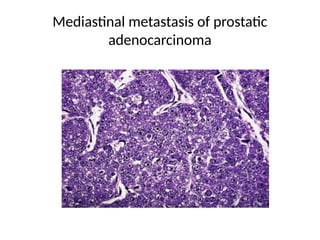
• Tumors that can metastasize to the
mediastinum and be confused with primary
neoplasms are
carcinomas of the breast, thyroid, nasopharynx,
larynx, kidney, prostate, and ovary testicular
germ cell tumors and malignant melanoma.