Introduction
• Affects bothlung compliance and lung expansion.
• Hallmark: Inability to increases lung volume in proportion to
pressure
• Reduction in surface area for gas diffusion causing ventilation
perfusion mismatch and hypoxia
4.
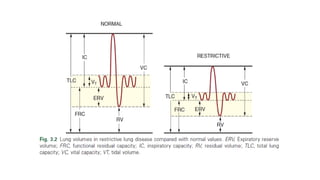
• Decrease inall lung volumes especially total lung capacity(TLC)
• Reduction of forced expiratory volume (FEV) in first second and
forced vital capacity (FVC)
• Normal to increased FEV1:FVC ratio
• Reduced diffusion capacity for carbon monoxide (DLCO)
5.
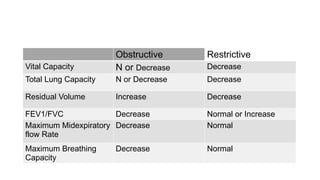
Obstructive Restrictive
Vital CapacityN or Decrease Decrease
Total Lung Capacity N or Decrease Decrease
Residual Volume Increase Decrease
FEV1/FVC Decrease Normal or Increase
Maximum Midexpiratory
flow Rate
Decrease Normal
Maximum Breathing
Capacity
Decrease Normal
8.
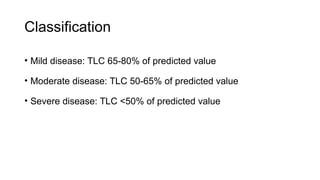
Classification
• Mild disease:TLC 65-80% of predicted value
• Moderate disease: TLC 50-65% of predicted value
• Severe disease: TLC <50% of predicted value
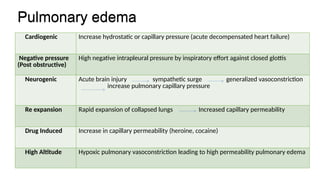
Pulmonary edema
Cardiogenic Increasehydrostatic or capillary pressure (acute decompensated heart failure)
Negative pressure
(Post obstructive)
High negative intrapleural pressure by inspiratory effort against closed glottis
Neurogenic Acute brain injury sympathetic surge generalized vasoconstriction
increase pulmonary capillary pressure
Re expansion Rapid expansion of collapsed lungs Increased capillary permeability
Drug Induced Increase in capillary permeability (heroine, cocaine)
High Altitude Hypoxic pulmonary vasoconstriction leading to high permeability pulmonary edema
Pulmonary edema
11.
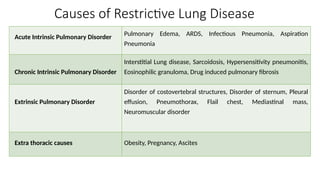
Extrinsic Restrictive LungDisease
Costovertebral skeletal deformity
• Compression of lungs, Decrease in compliance
• Increase stiffness and decrease in TLC
• Raised hemidiaphragm on the side of convexity
• 2 Basic type of costovertebral deformity
oKyphosis
oScoliosis
12.
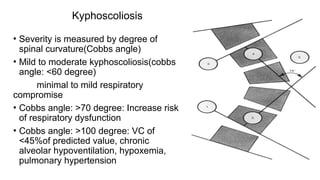
Kyphoscoliosis
• Severity ismeasured by degree of
spinal curvature(Cobbs angle)
• Mild to moderate kyphoscoliosis(cobbs
angle: <60 degree)
minimal to mild respiratory
compromise
• Cobbs angle: >70 degree: Increase risk
of respiratory dysfunction
• Cobbs angle: >100 degree: VC of
<45%of predicted value, chronic
alveolar hypoventilation, hypoxemia,
pulmonary hypertension
13.
Obesity
• Restricting diaphragmaticmotion
• Each kg gain in weight :26 cc of VC ↓
• Decrease in FEV1, FVC and ERV
• BMI >40kg/m2: Decrease in TLC and residual volume
• Severe Overweight BMI >44: expiratory flow limit and
generation of intrinsic auto PEEP and v/q mismatch
14.
Preoperative Assessment
• Assessmentof the severity of lung disease
• Optimization of preoperative status
• Identification and management of treatable issues
Physical Examinations
• Signsof Hypoxemia and Hypercapnia, Increase work of
breathing
• Clubbing
• BMI
• External Deformity of spine, chest wall
• Lung Ascultation for presence of crackles
• Baseline spo2 at rest and exertion
17.
Investigations
• Chest Xray: Opacities, fluid overload, effusion, pneumothorax
• Echocardiography: In a patient with a worsening symptoms, To
rule out the pulmonary artery hypertension
• ABG Analysis: To look for the hypoxemia and hypercapnia
Paco2 >45mmHg: postoperative pulmonary complication
18.
• CT Scan:
oTodiagnose and look for the progression of ILD
oSize of mediastinal mass and degree of tracheal compression
• Spirometry:
oType and severity of respiratory impairment, for the prolonged ventilatory
support
oInterstitial Lung disorder have decrease TLC, FRC, RV, FVC
oSevere Obesity : Decrease FEV1
19.
• Diffusion capacityfor carbon monoxide
o Gas exchange capacity of lungs
o Total functioning surface area of alveolar capillary interface
o Also used to predict the postoperative pulmonary complication
post lung resection(<40%)
20.
• Six minutewalk test
↓Spo2 >4% ↑risk of complication
21.
Preoperative Management
Acute IntrinsicPulmonary Disorder
• Postponed of elective surgery for patient with acute pulmonary
disease and active infection
• Treatment of untreated hypoxemia, Underlying disease and
active infection
• Diuretics if fluid overload, heart failure
• Drainage of large pleural effusion and ascites
22.
Chronic Intrinsic PulmonaryDisorder
• Cessation of smoking for at least 8 weeks before surgery
• Pulmonary Rehabilitation and physiotherapy
• Avoidance of exposures such as drugs, asbestos, silica
• Weight reduction: 10% decrease in weight cause 20% increase in exercise
duration
• Preoperative radiation to reduce size of malignant mediastinal mass
23.
Perioperative medical management
•Management of restrictive disease varies on etiology
• Interstitial lung disease : Immuno suppresant drugs like
steroids, cyclophosphamide, methotrexate; Antifibrotic drugs
like nintedanib, pirfdenidone
• Patient with acute exacerbations treated with antibiotics, steroid
24.
• Antifibrotics andimmunosupressant drugs shows to improve the
pulmonary function so advised to postpone the surgery in
patients having them
• Steroids are used in lowest possible dose in the perioperative
period due to suppression of HPA axis
• Immuno suppresent drugs are continued in current dose
through out perioperative period
• Immunosuppresent like methotrexate can cause leucopenia,
thrombocytopenia
25.
Intraoperative Management
• Selectionof anesthetic techniques and anesthetic agents
• Positioning of the patients
• Induction and airway management
• Ventilatory management
26.
Regional Block
• Forselective patients and surgical procedure
• Surgical anesthesia and post operative analgesia
• Minimal sedation and opoids administration
• Risk of respiratory complications less
27.
Brachial Plexus Block
•Interscalene block
oBlock of phrenic nerve causing hemidiaphragmatic paralysis 100%
oReduction of FEV1 and FVC
oRisk of Pneumothorax
• Supraclavicular Block and Infraclavicular Block
o Under USG guidance due to risk of pneumothorax(0.5-6%)
oPhrenic Nerve block( 40-60%)
28.
Neuraxial Anesthesia
• Intraoperativesurgical anesthesia and postoperative analgesia
• Effects depending on extent of motor blockade
• High neuraxial technique reduces inspiratory capacity ,
expiratory reserve volume
General Anesthesia
• Impairmentof arterial oxygenation increased If associated with smoking,
obesity and pulmonary hypertension
• Preoxygenation: Passive oxygenation using nasal cannula at 10l/min with
100% oxygen via facemask
• Use of nasal cannula during laryngoscope
• Use of high flow nasal cannula: Increase nasopharyngeal airway pressure
at the end of expiration causing peep effect and enhance oxygenation.
31.
• Induction inhead up position than supine position when moderate to
severe restriction or orthopnea
• Awake intubation if associated with severe restriction and a
potentially difficult airway
• Avoidance of long acting opioids and sedative agents
• Inducing agents such as propofol, ketamine can be used because of
broncho dilatory effects
32.
• Volatile inhalationalagents : Bronchodilator effects
(sevoflurane>>Halothane>> Isoflurane>>Desflurane
• Controlled ventilation via ET tube to optimize oxygenation and
ventilation
• Administration of neuromuscular blocking agents (TOF)and
adequate anesthetic depth to minimize airway pressure
33.
• Avoidance ofbarotrauma and acute lung injury
• Use of long duration of inspiration compared to expiration
(1:1 to 1:1.5), small tidal volumes
• Increase in respiratory rate to maintain paco2 with pH 7.35-7.45
(Lung protective ventilation)
• FiO2 and PEEP adjusted to maintain spo2>90%, paO2>60mmHg
• Initially PEEP of 5cm H2O is used which can be cautiously
increased to 12cm H2O
34.
Extubation
• Extubation inreverse Trendelenburg position
• Patient is alert, cooperative and without signs of respiratory
distress
• Guidelines indicating successful extubation :
oVital capacity >15ml/kg
oPao2 >60mmHg with FiO2 <0.5
oNegative inspiratory pressure >-20cm H2O
oNormal pH
oRespiratory rate <20 breaths/min
35.
Intraoperative complications
• Hypoxemia:
oV/Qmismatch and shunt: Atelectasis or intrapulmonary shunt ,
Increase PEEP, Administration of inhaled pulmonary vasodilators
oCompression of lungs: Changing position
oInadequate ventilation: Tube blockage, Tube displacement
• Impaired diffusion:
Pulmonary hypertension, severe fibrotic interstitial lung disease
Decrease in diffusion area and perfusion time
Increase in intraoperative fio2
36.
• Pneumothorax andpulmonary embolism
Cause sudden hypoxemia and severe hypotension
Treated by emergency needle decompression and chest tube
placement
• Arrhythmia
Due to hypoxia, hypercapnia or acid base imbalance
Prompt diagnosis and treatment of underlying cause along with
anti arrhythmia may be indicated
37.
• Exacerbation ofpulmonary hypertension
Due to hypoxemia, hypercapnia, acidosis, hyperthermia, nitrous
oxide and high PEEP
Treated with supplemental oxygen, diuretics, Ionotropic agents
Inhalational agents also cause inhibition of hypoxic pulmonary
vasoconstriction
38.
Post Anesthetic Careunit management
• Respiratory distress
• Ensuring adequate analgesia
• Deep breathing exercise, lung expansion, coughing and early
mobilization to prevent atelectasis
• Use of CPAP or HFNC to reduce work of breathing, respiratory
rate and for treatment of hypoxemia
39.
Summary
• RLD affectboth lung expansion and compliance and cause
decrease in lung capacities
• Preoperative assessment and optimization is done
• Regional anesthesia is preferred over GA
• Use of various measures to prolong the apneic period
• Use of inducing and inhalational agents with bronchodilators
properties
• Lung protective ventilation strategy
• Proper post operative analgesia and management
#13 Increased weight of chest wall and increase abd adipose tissue
due to compression of small airways
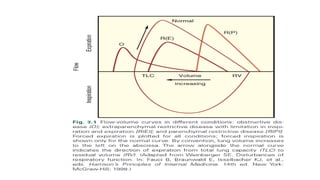
#19 Distinguish between intrinsic lung disease in which it is decreased to other cause of restrictive lung disease
#27 Regional nerve block in anesthesia and pain therapy by danilo jankovic
#29 Surgical positioning during anesthesia : significant physiological effect on ventilation, perfursion, intrathoracic pressure, exaggerataed in RLD
Lateral: Dependent lung: v/q mismatch, severe impairment in oxygenation, causing increase in fio2, applyimg peep may improve oxygenation by reducimg atelectasis
Sitting position low intrathoracaic pressure, absominal content fall away from diaphragm increasing in frc, lung compliance
Trendelenburg: Cephalad movement of viscera against diaphragm, Increase venous return
#30 Arterial oxygenation is impaired in GA and more in RLD and condition which impair gas exchange
Passive oxygenation done to prolong the apneic time during laryngoscopy and intubation
Use of hfnc to increase high arterial oxygen tension
#31 Head up position can optimize frc, preserving lung compliance and reducing work of breathing
Awake intubation to avoid the period of apnea
Opioids diminish the respiratory drive and cause respiratory depression( morphine, hydromprphone)
Inducing agents increase the sympathetic tone
#32 Controlled ventilation as pt with interstitial lung disease has increased risk of ventilator induced lung injury
#33 Decrease lung compliance results in high peak inspiratory pressure during positive pressure ventilation causing increase in risk of volutrauma and barotrauma
High PEEP increase intrathoracic pressure impairing venous return, decrease cardiac output and hypotension
Low tidal volume can result in respiratory acidosis which can be avoided by increase in rr , reducing dead space by shortening ventilatoru tubing
Spo2 100% is avoided to prevent the absorption atelectasis
Peep increase to improve oxygenation but high peep cause inc. intrathoracic pressure causing decrease venous return, cardiac output and subsequently hypotension
Redistribution of blood away from aerated lung to atelectataic lung worsening v/q mismatch
#35 The most common cause of hypoxemia is v/q mismatch which is usually due to atelectasis leading to intrapulmonary shunting not responding to increase in fio2
Pulmonary vasodilators nitric oxide
Impaired diffusion seen in pt with pulmonary htn
#38 Monitoring of respiratory distress
Ensuring adequate analgesia to facilitated the cough and deep breath





















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















