Download as PDF, PPTX

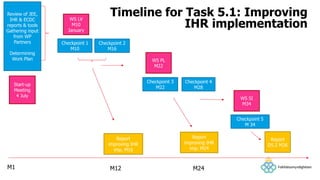

The document outlines the efforts of the Public Health Agency of Sweden to strengthen IHR implementation and assess public health preparedness in low GNI countries. It discusses three main tasks focused on improving collaboration during crises, conducting assessments through workshops and evaluations, and identifying areas for improvement in health systems. The document highlights specific countries involved, key findings from assessments, and planned actions to enhance preparedness and response capabilities across member states.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





