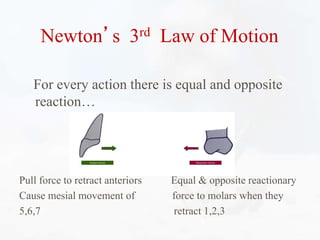
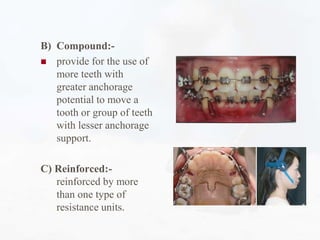
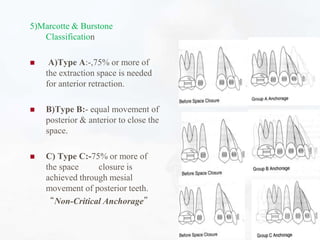
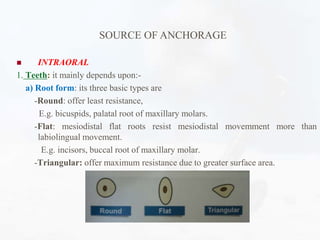
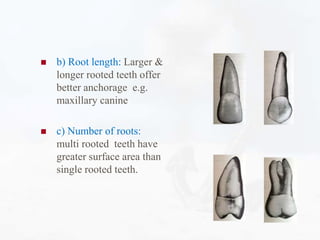
Anchorage refers to resistance to unwanted tooth movement when orthodontic forces are applied. There are various sources of anchorage, including teeth, bone, implants, and extraoral appliances. Anchorage preparation involves incorporating multiple teeth, using reinforcing appliances, and positioning teeth at right angles to forces to maximize resistance. Proper anchorage planning considers the anchorage demand based on the number and type of teeth to be moved and duration of treatment.
























































![lecture_05_and_06-Anchorage_in_orthodontics[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture05and06-anchorageinorthodontics1-240224004209-047377b5-thumbnail.jpg?width=640&height=640&fit=bounds)
























