Downloaded 646 times
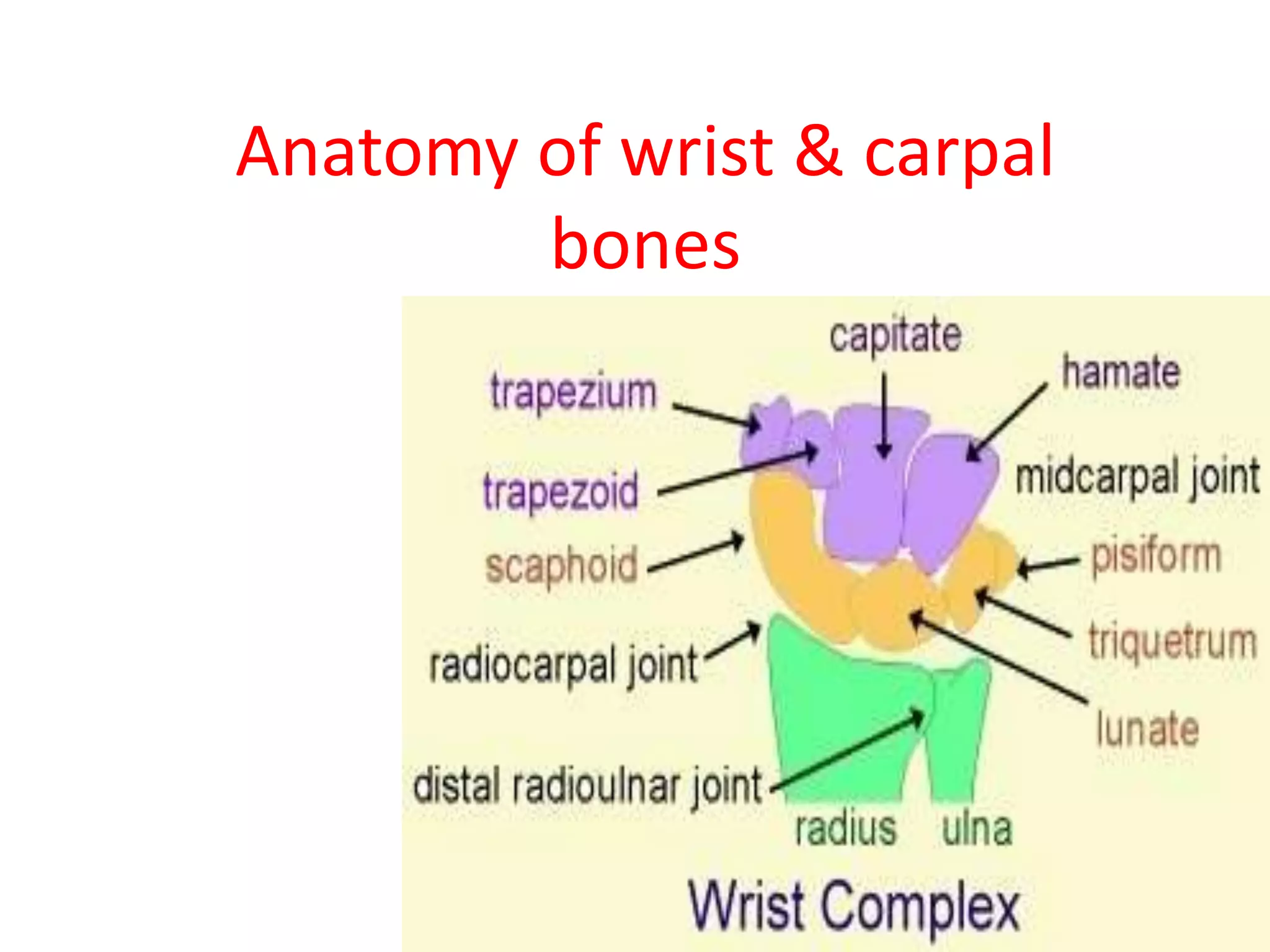


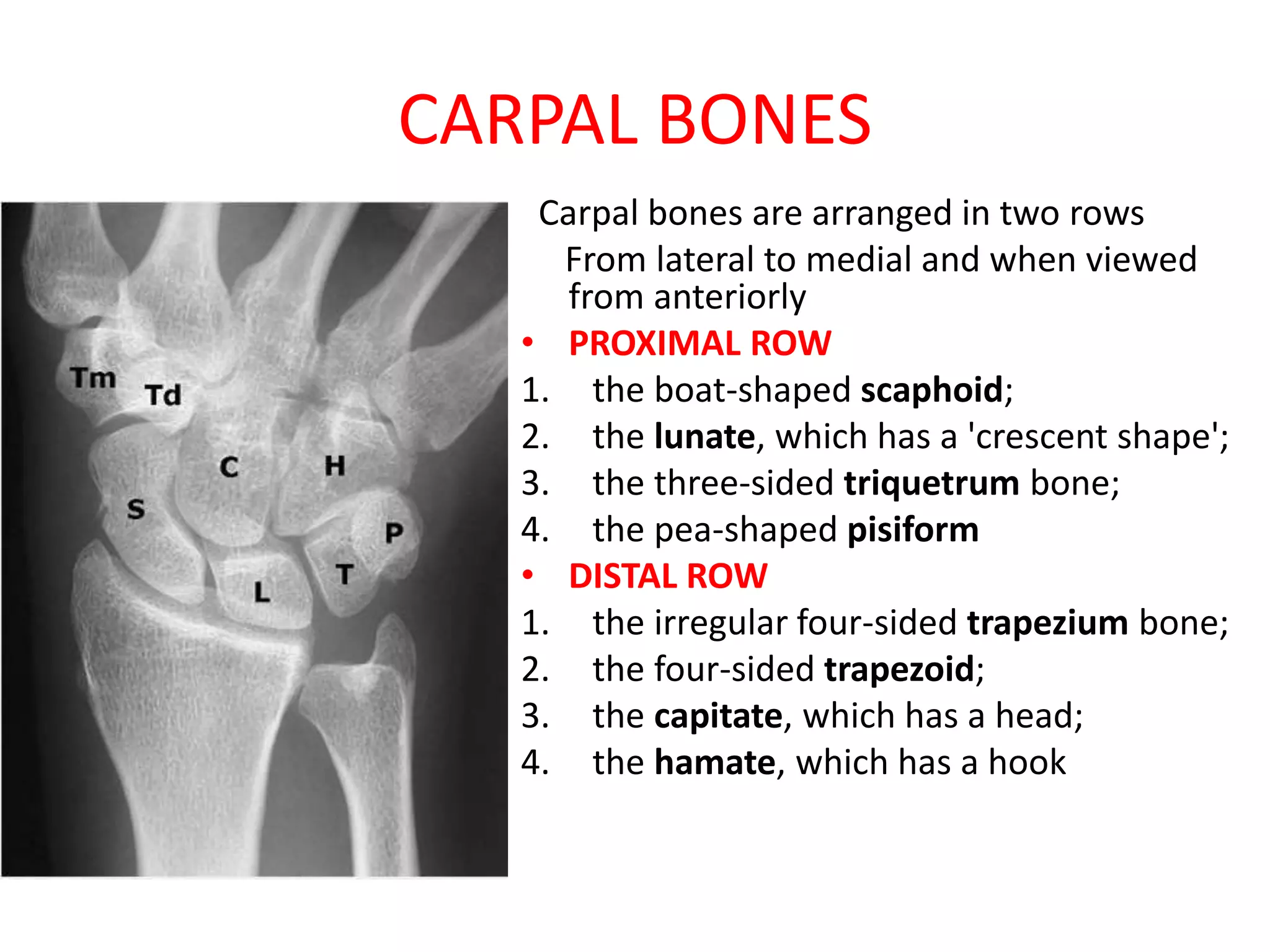










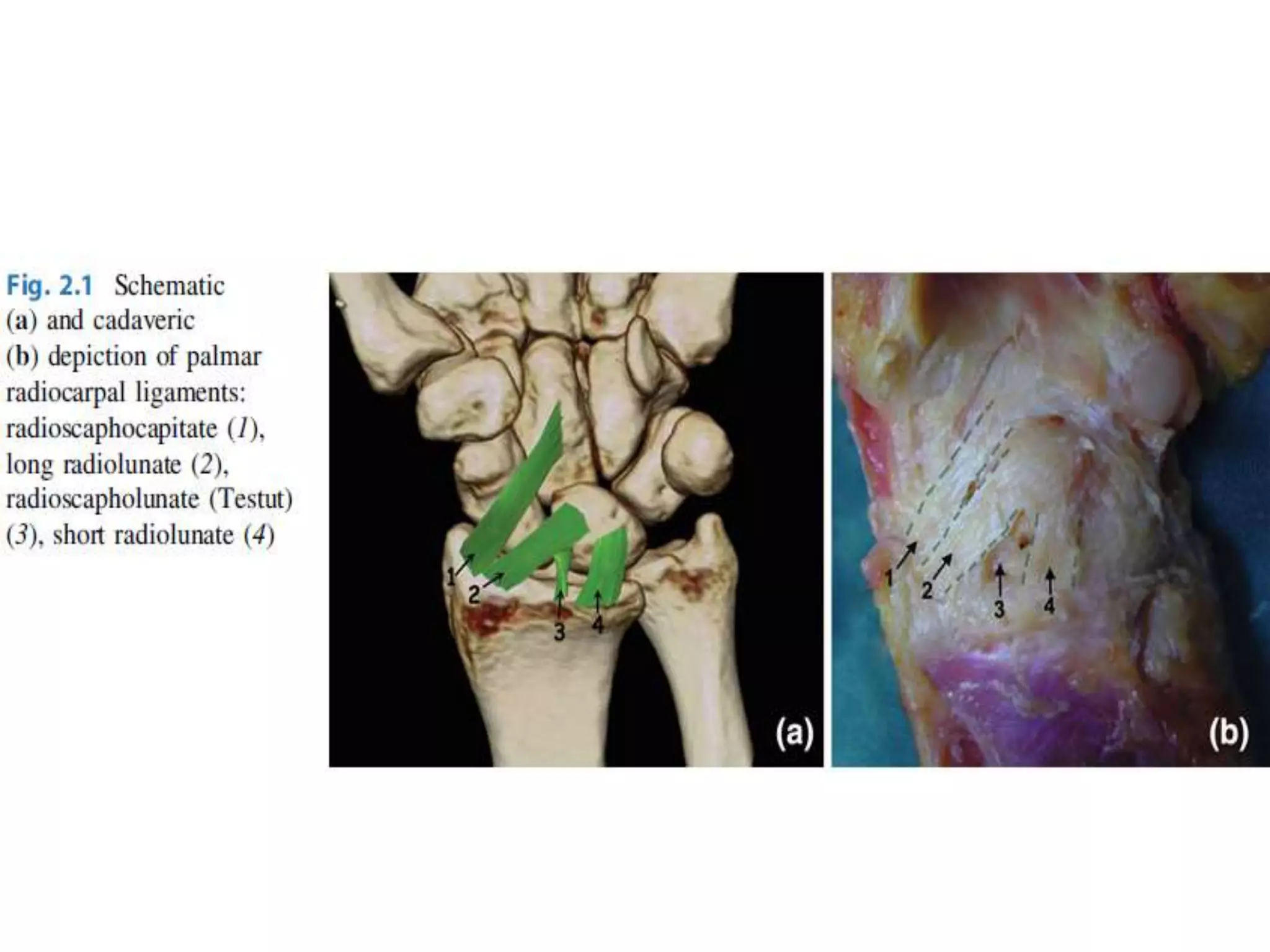



























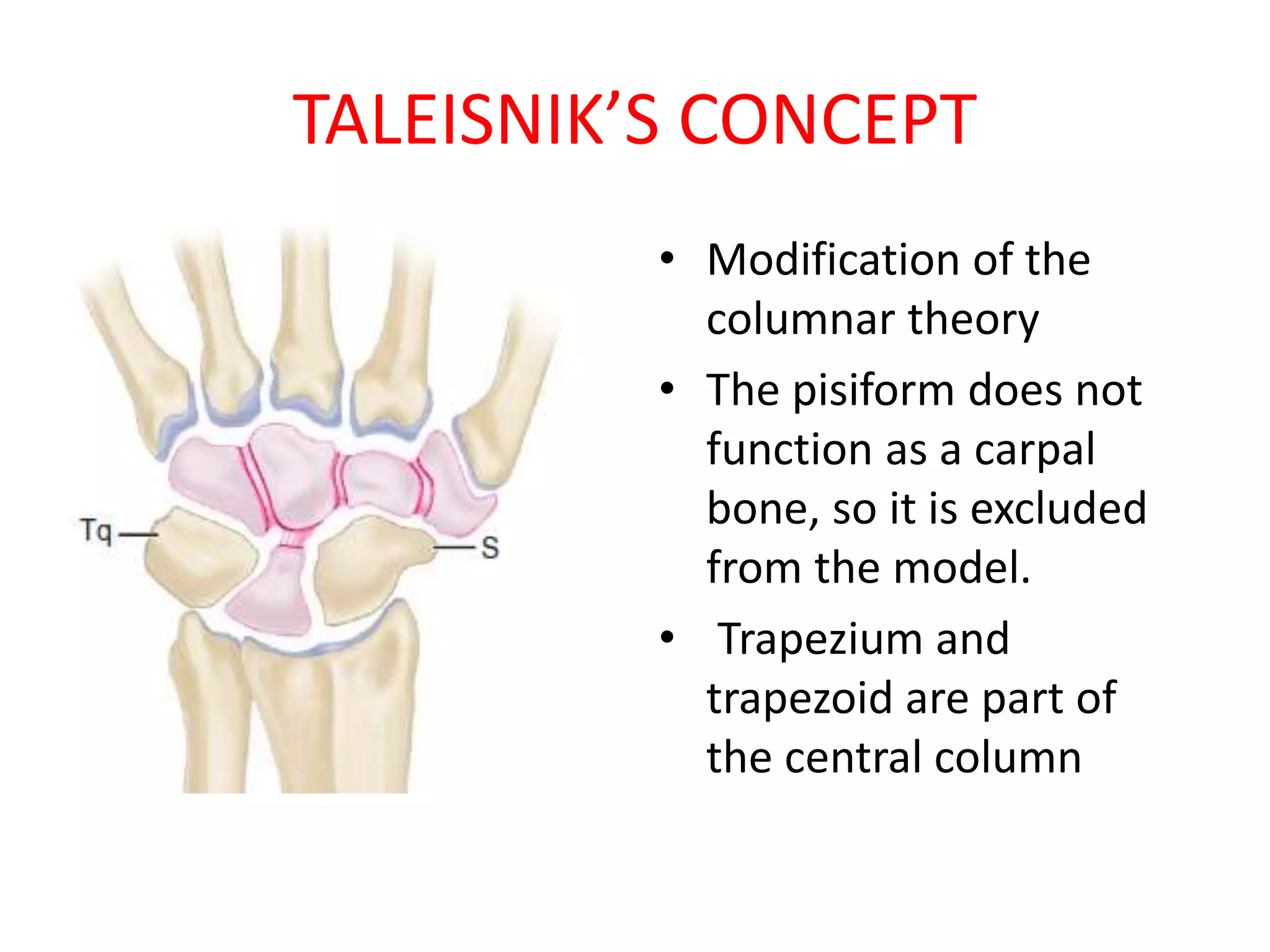











The document provides details on the anatomy of the wrist and carpal bones. It can be summarized as: 1. The wrist joint is made up of the distal ends of the radius and ulna articulating with the proximal and distal rows of carpal bones, which then articulate with the metacarpal bones. 2. The carpal bones are arranged in two rows - the proximal row includes the scaphoid, lunate, triquetrum, and pisiform bones. The distal row includes the trapezium, trapezoid, capitate, and hamate bones. 3. The carpal bones are stabilized by intrinsic and extrinsic ligaments including the scapholunate and


















![2. shoulder joint & its applied anatomy 07[1]](https://cdn.slidesharecdn.com/ss_thumbnails/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




































































