Downloaded 336 times

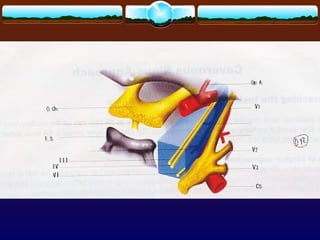
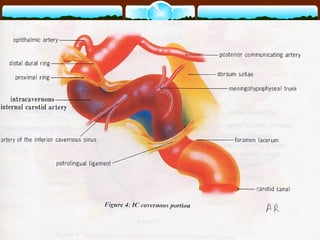
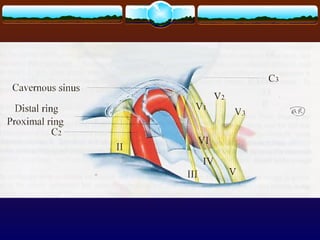
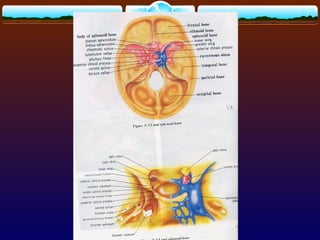
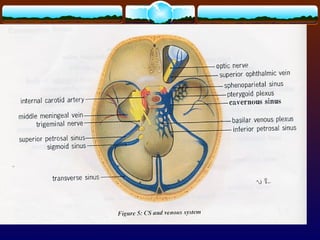
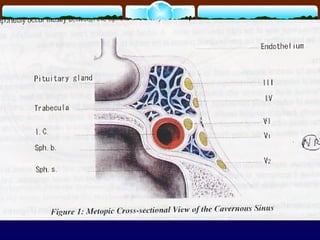
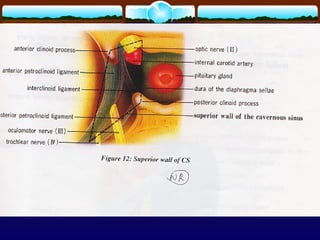

This document discusses the anatomy of the cavernous sinus (CS). It describes the CS as being located on either side of the sella turcica and extending from the sphenoid fissure to the petrous apex. It contains the internal carotid artery as well as cranial nerves III, IV, V1 and V2. The CS drains into the inferior petrosal sinus and receives blood from various veins including the sphenoparietal sinus and ophthalmic veins. The document discusses the osseous structures surrounding the CS and details the arterial, venous and neural compartments within the sinus.
















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















