Downloaded 27 times










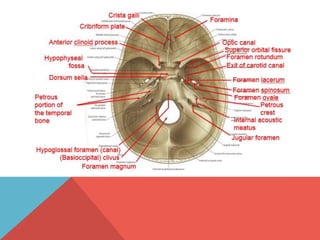























































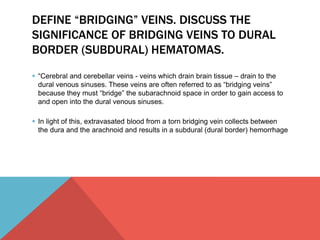








































































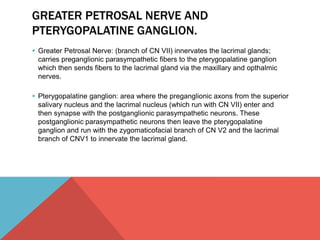
![WHAT STRUCTURES PASS THROUGH THE
SUPERIOR ORBITAL FISSURE AND SUPERIOR
ORBITAL FORAMEN
Superior Orbital Fissure:
oculomotor nerve (cranial nerve [CN] III),
trochlear nerve (CN IV),
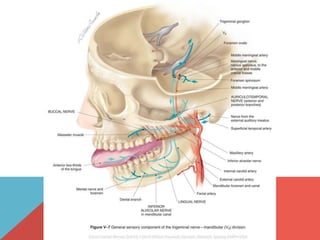
ophthalmic nerves (branches of the ophthalmic division of the trigeminal
nerve [CN V1),
abducens nerve (CN VI), and
superior ophthalmic vein
Superior orbital foramen
supraorbital branch of opthalmic nerve,
supraorbital artery, and
superior ophthalmic vein](https://image.slidesharecdn.com/mbbanatomy-141117134341-conversion-gate01/85/MBB-Anatomy-221-320.jpg)







































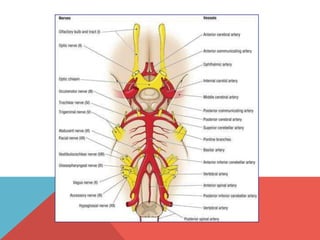
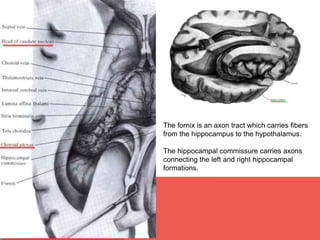
This document provides terminology and descriptions related to the anatomy of the head and neck. It discusses the compartments of the cranial cavity, orbits, ear, nose, and oral cavity. It then describes the deep muscular, visceral, and carotid sheath compartments of the neck. Finally, it lists synovial joints in the head including the temporomandibular joint, atlanto-occipital joints, and interossicular joints of the middle ear.





































































































