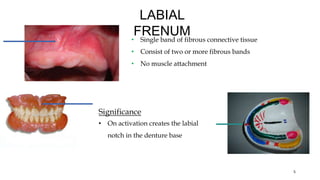
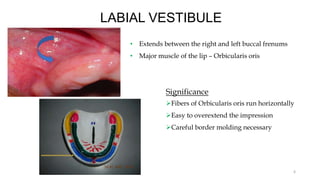
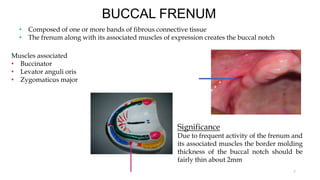
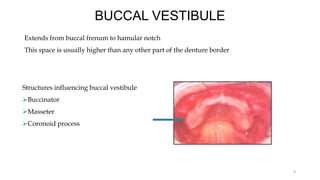
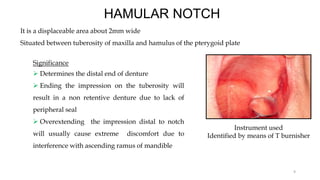
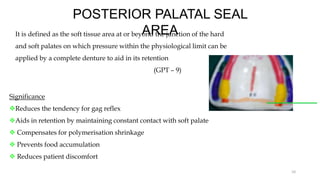
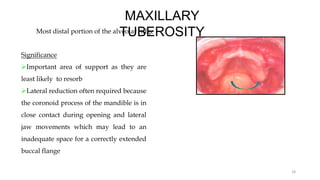
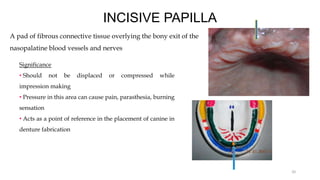
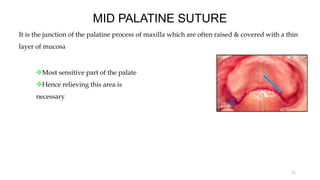
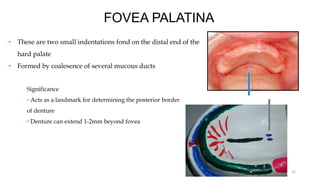
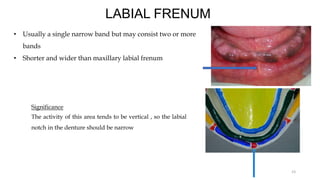
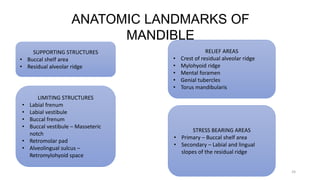
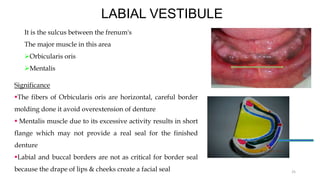
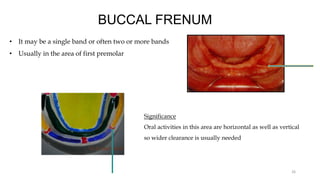
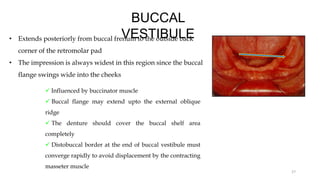
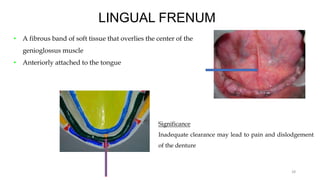
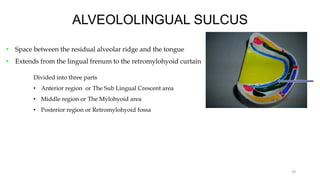
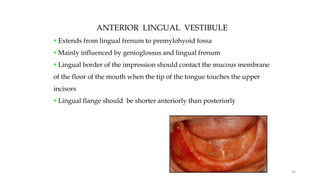
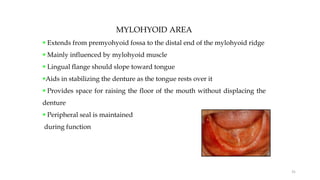
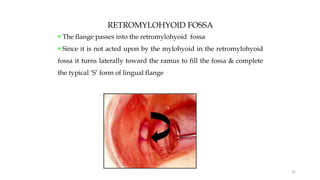
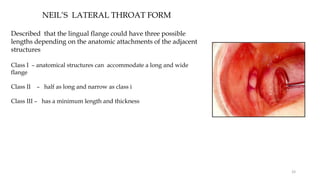
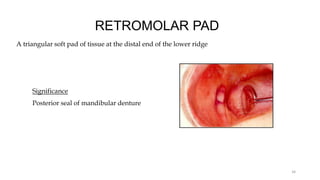
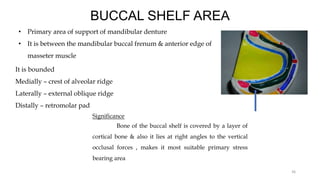
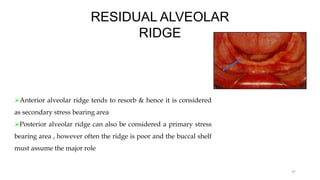
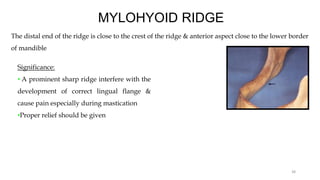
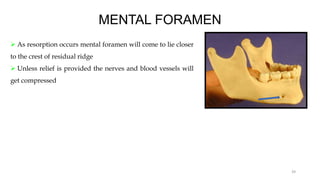
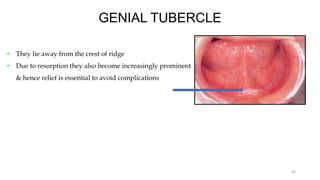
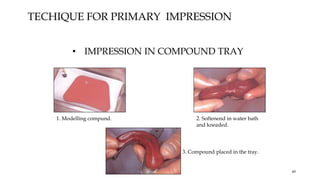
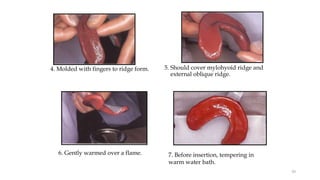
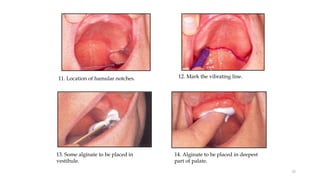
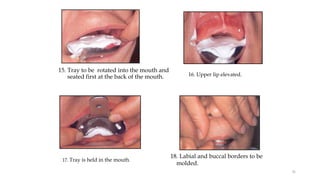
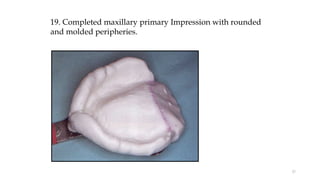
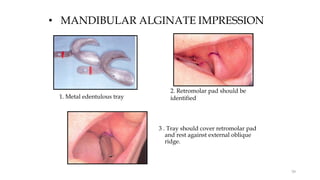
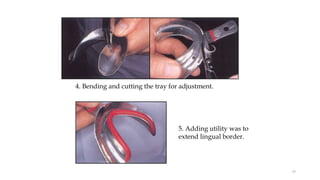
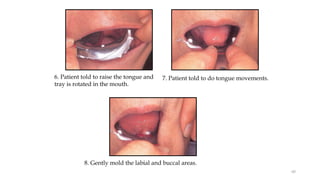
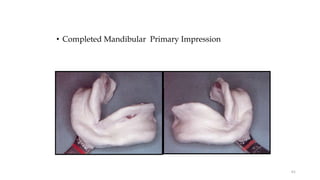
This document discusses anatomical landmarks that are important for making impressions for complete dentures. It describes landmarks in the maxilla like the hard palate, rugae, maxillary tuberosity, incisive papilla, and fovea palatine which provide support or need relief. Limiting structures like the labial and buccal frenums are also outlined. For the mandible, supporting areas include the buccal shelf and residual ridge while the mylohyoid ridge and mental foramen require relief. The principles of impression making and objectives of obtaining retention, stability and support are reviewed. Techniques for primary impressions using compound or alginate are demonstrated.