Downloaded 344 times












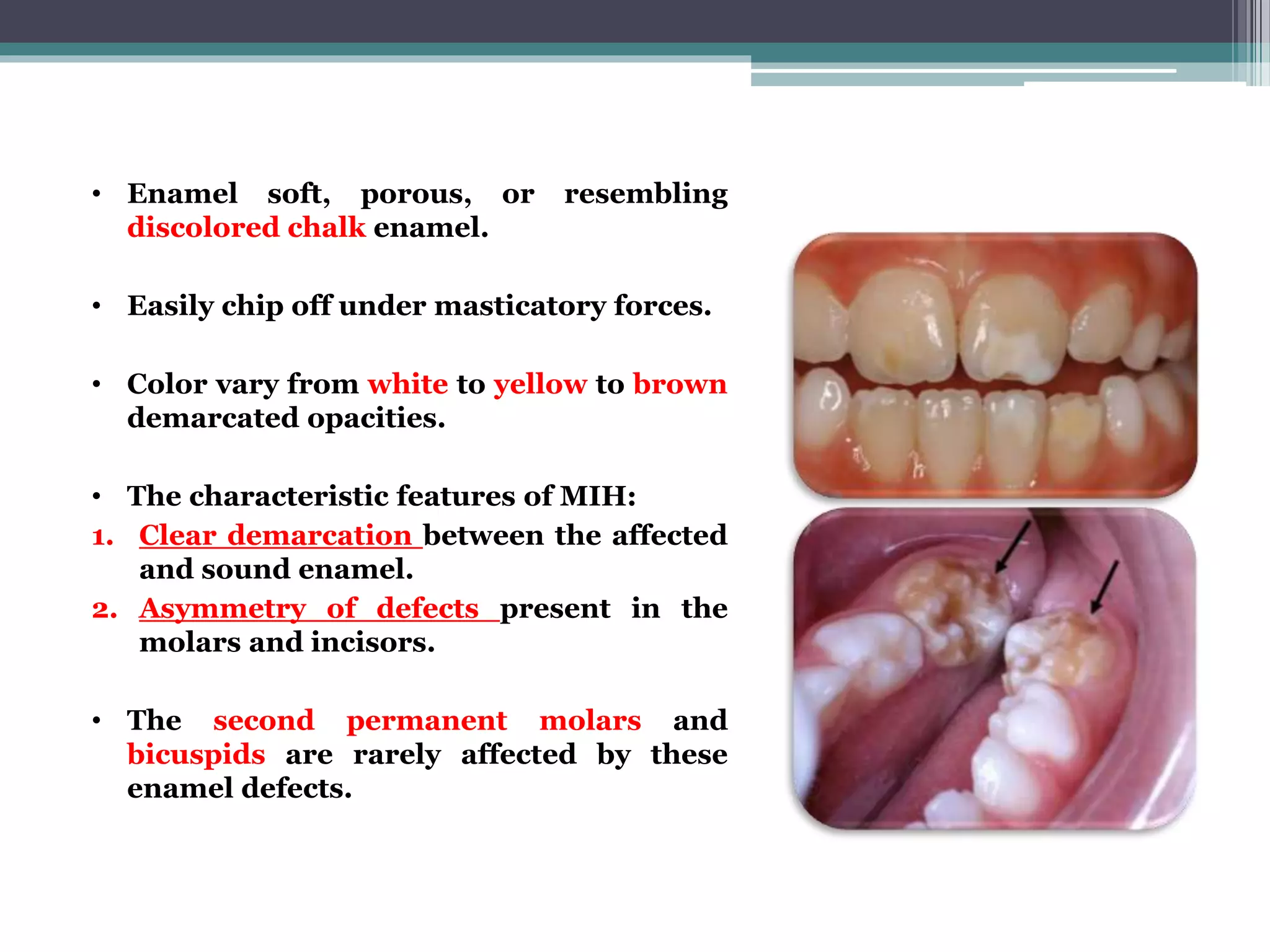


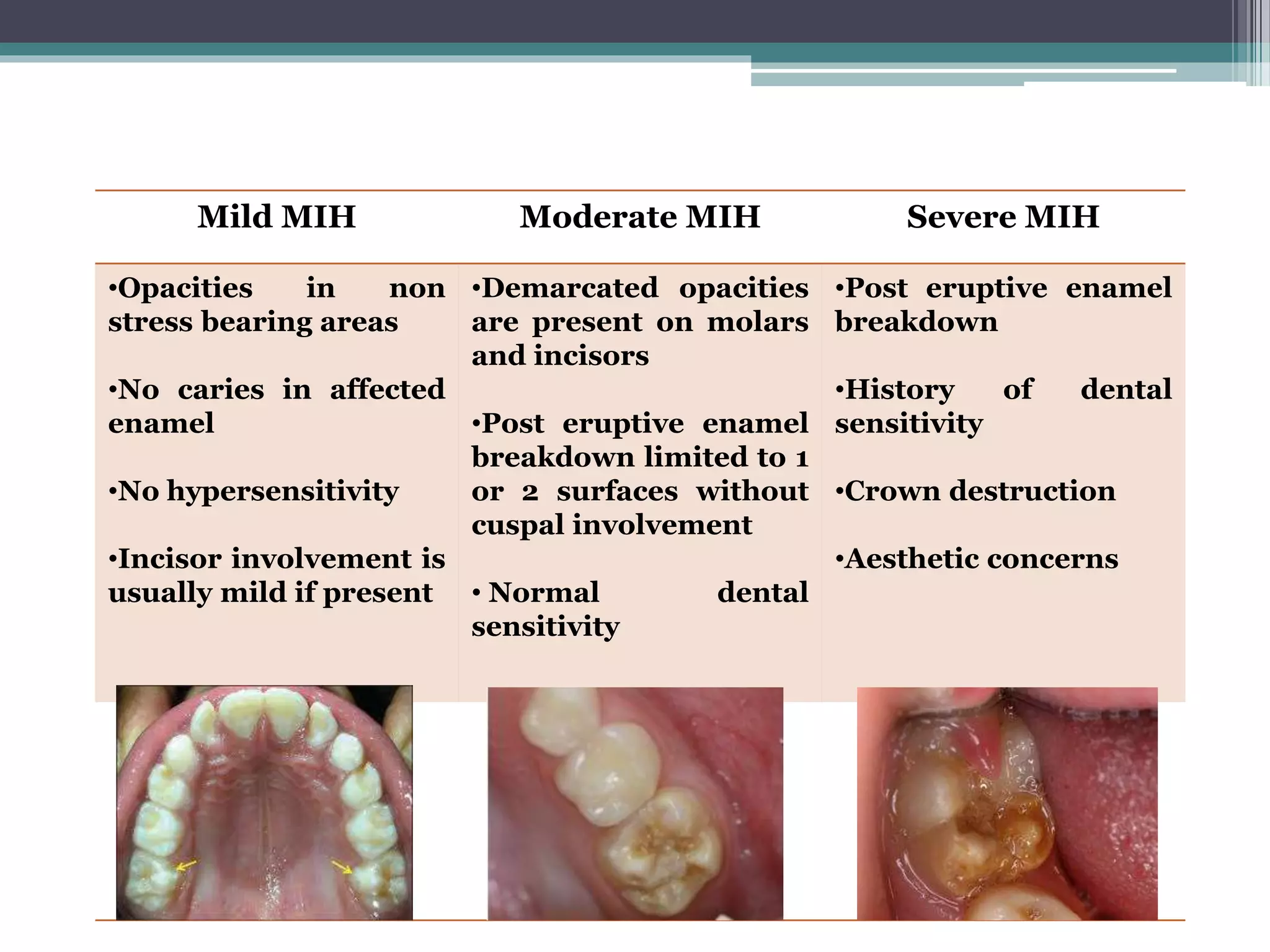


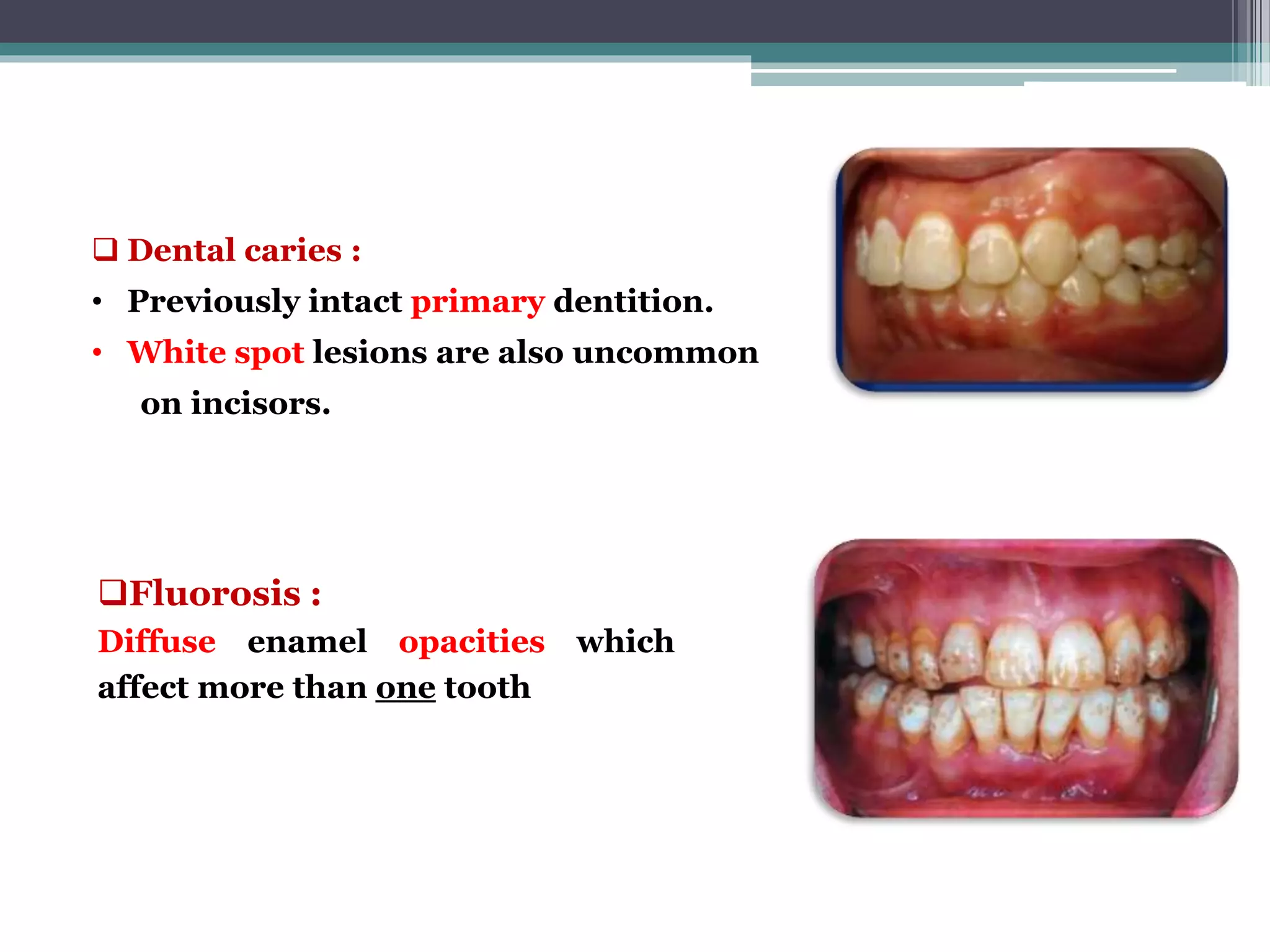
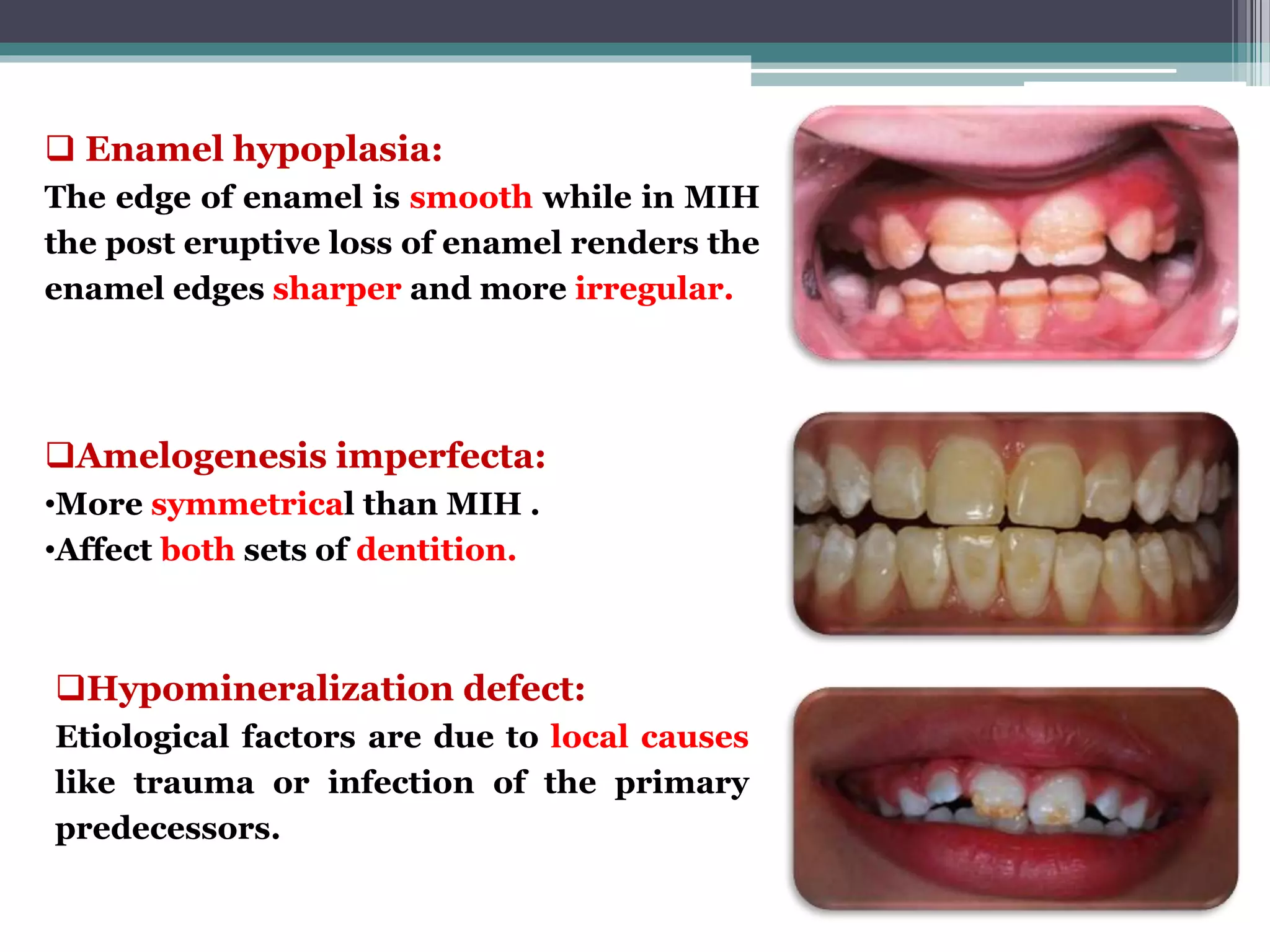

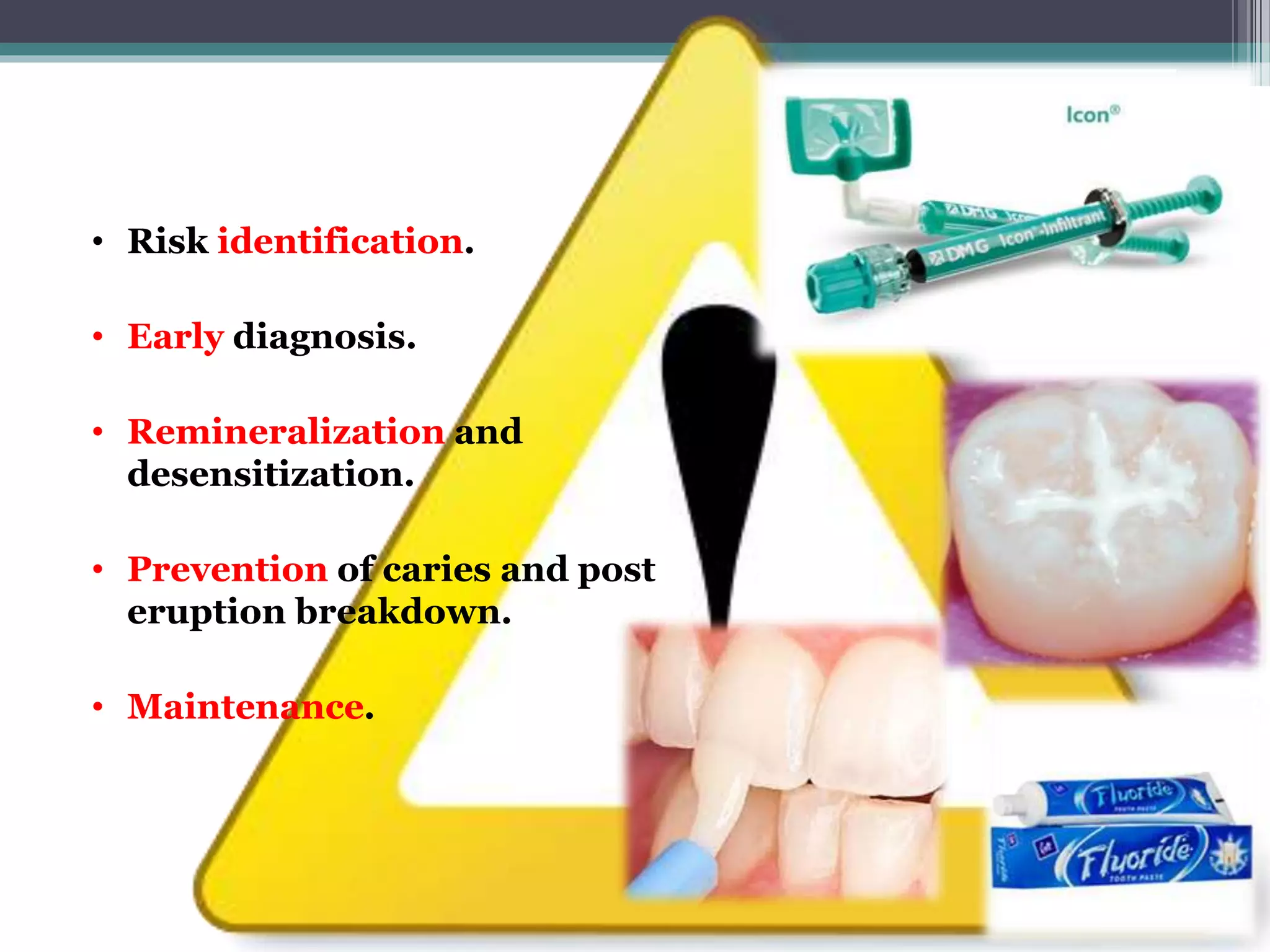
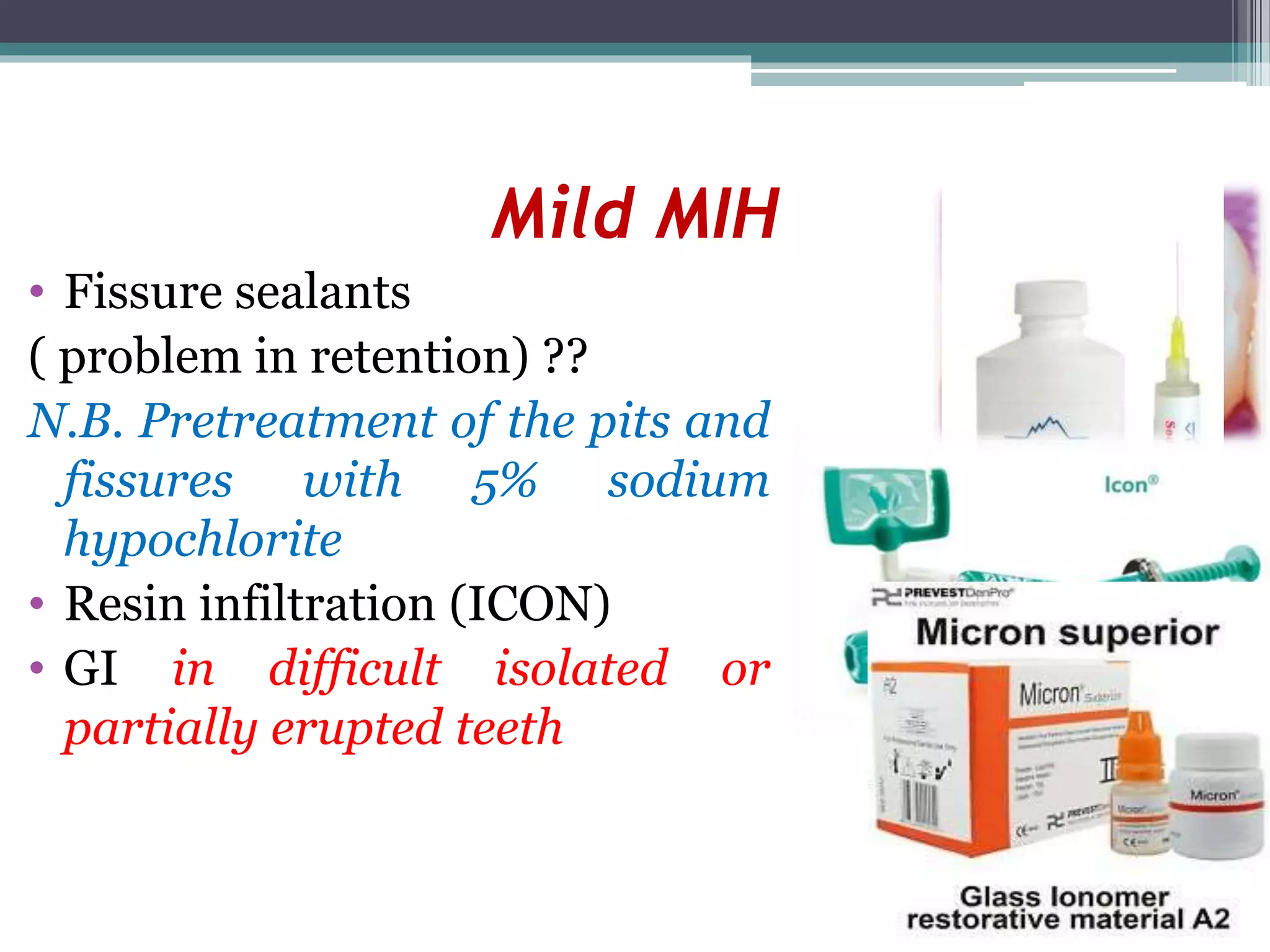








The document discusses molar incisor hypomineralization (MIH), a qualitative defect of enamel characterized by its hypomineralization and association with first permanent molars and incisors. It covers the etiology, prevalence, clinical problems, diagnostic criteria, severity, differential diagnosis, prevention, and treatment of MIH. The prognosis of affected teeth is generally poor due to the compromised enamel quality supporting restorations.



































































