Downloaded 72 times



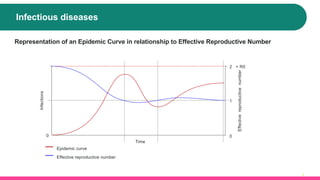
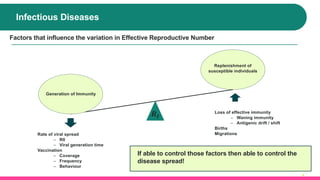





The document presents an introduction to infectious disease modeling, emphasizing the importance of infectious diseases and how mathematical modeling can aid in understanding and controlling their spread. It outlines the differences between static and dynamic models based on their impact on transmission and discusses various factors influencing the effective reproductive number. Furthermore, it highlights a case study involving dynamic transmission cost-effectiveness modeling for childhood influenza vaccination, demonstrating the advantages of accounting for indirect effects in health-economic analysis.