Downloaded 13 times

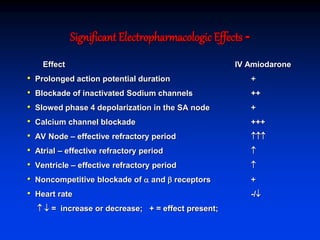
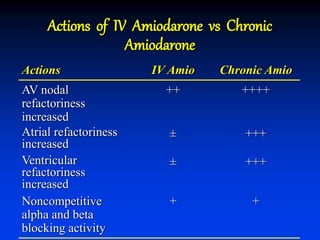



- Amiodarone is a class III antiarrhythmic agent with alpha, beta, sodium, potassium, and calcium channel blocking properties. It is indicated for ventricular and atrial dysrhythmias. - Amiodarone has a long half-life, can be used in patients with kidney failure on dialysis, is generally well tolerated even in advanced heart failure, and has a very low risk of torsades de pointes. - The mechanism of action of amiodarone includes prolonging the action potential duration and effective refractory periods while also having anti-sympathetic effects through alpha and beta receptor blockade.




































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















