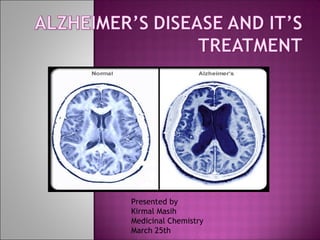
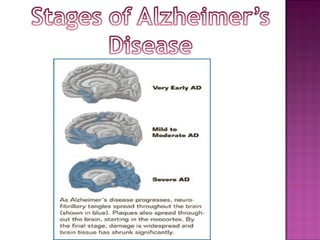
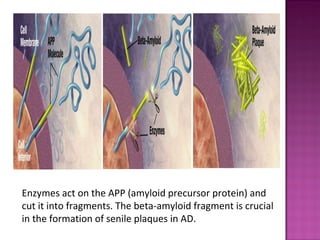
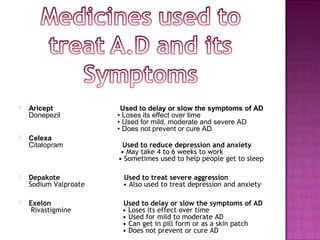
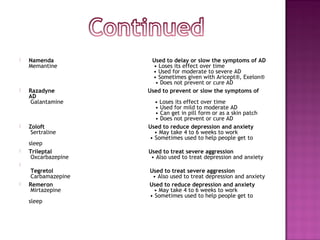
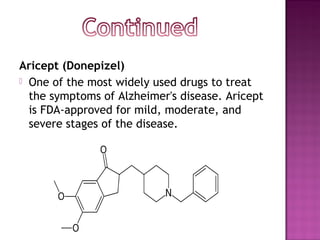
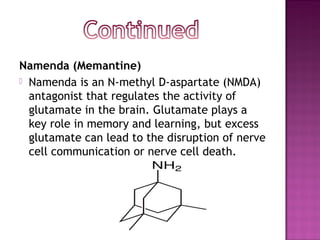
This document discusses Alzheimer's disease, including its causes, symptoms, stages of progression, diagnosis, current treatments, and potential new treatments in development. Specifically, it describes how Alzheimer's is characterized by beta-amyloid plaque and tau protein tangle buildup in the brain, outlines the four stages of the disease and their symptoms, and discusses several FDA-approved medications commonly used to treat symptoms, including Aricept, Exelon, Razadyne, and Namenda. It also mentions two new compounds in clinical trials, a beta-secretase inhibitor and NIC5-15, that may help slow the disease's progression.