Downloaded 503 times
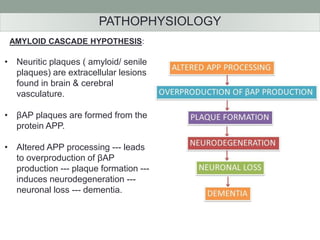
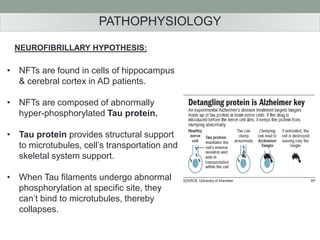
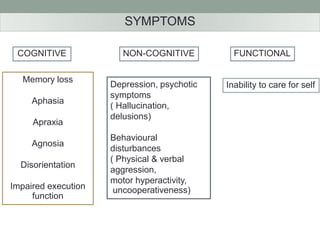
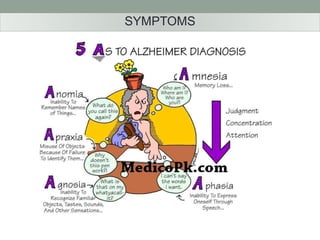
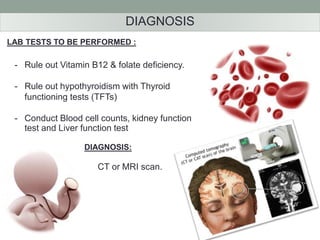
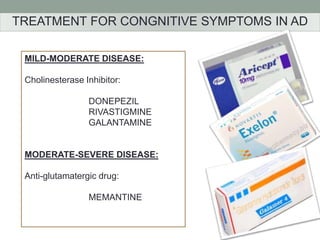
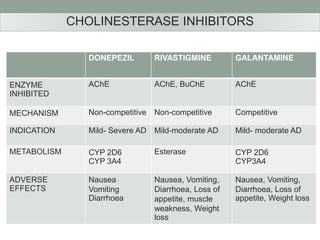
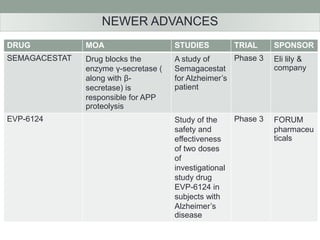

This document summarizes information about Alzheimer's disease from a student paper, including descriptions of symptoms, causes, pathophysiology and treatment options. It discusses how Alzheimer's is a progressive neurodegenerative disorder causing dementia. Key pathological features are amyloid plaques and neurofibrillary tangles in the brain. Current treatments aim to improve cognitive symptoms and include cholinesterase inhibitors such as donepezil for mild-moderate cases and memantine for moderate-severe cases. Several drug trials are also mentioned.


























![Parkinson's Disease [Advanced Pharmacology]](https://cdn.slidesharecdn.com/ss_thumbnails/07-210419085948-thumbnail.jpg?width=640&height=640&fit=bounds)








































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





