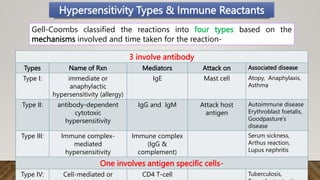
This document discusses different types of hypersensitivity reactions and allergies. It describes 4 types of hypersensitivity reactions:
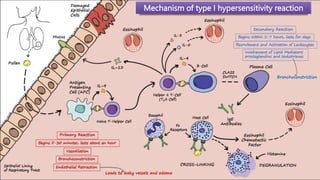
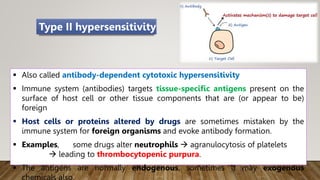
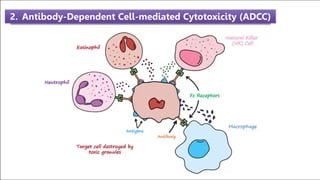
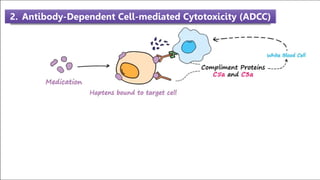
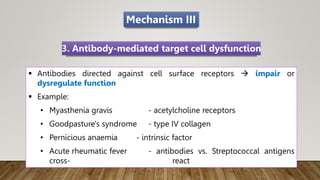
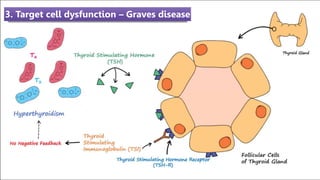
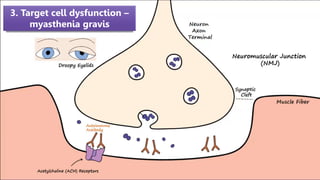
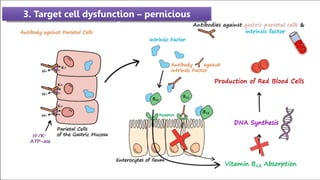
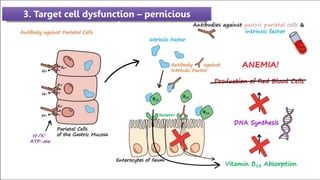
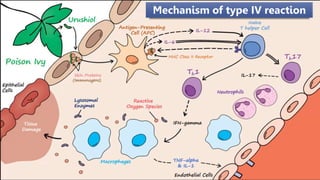
Type I is an immediate or anaphylactic reaction mediated by IgE antibodies and mast cells. Type II involves antibody-dependent cytotoxic reactions mediated by IgG and IgM antibodies. Type III reactions are immune complex-mediated responses. Type IV is a cell-mediated reaction involving T cells. The document provides details on the mechanisms, mediators, symptoms and treatments for each type of hypersensitivity reaction.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











