Download as PDF, PPTX
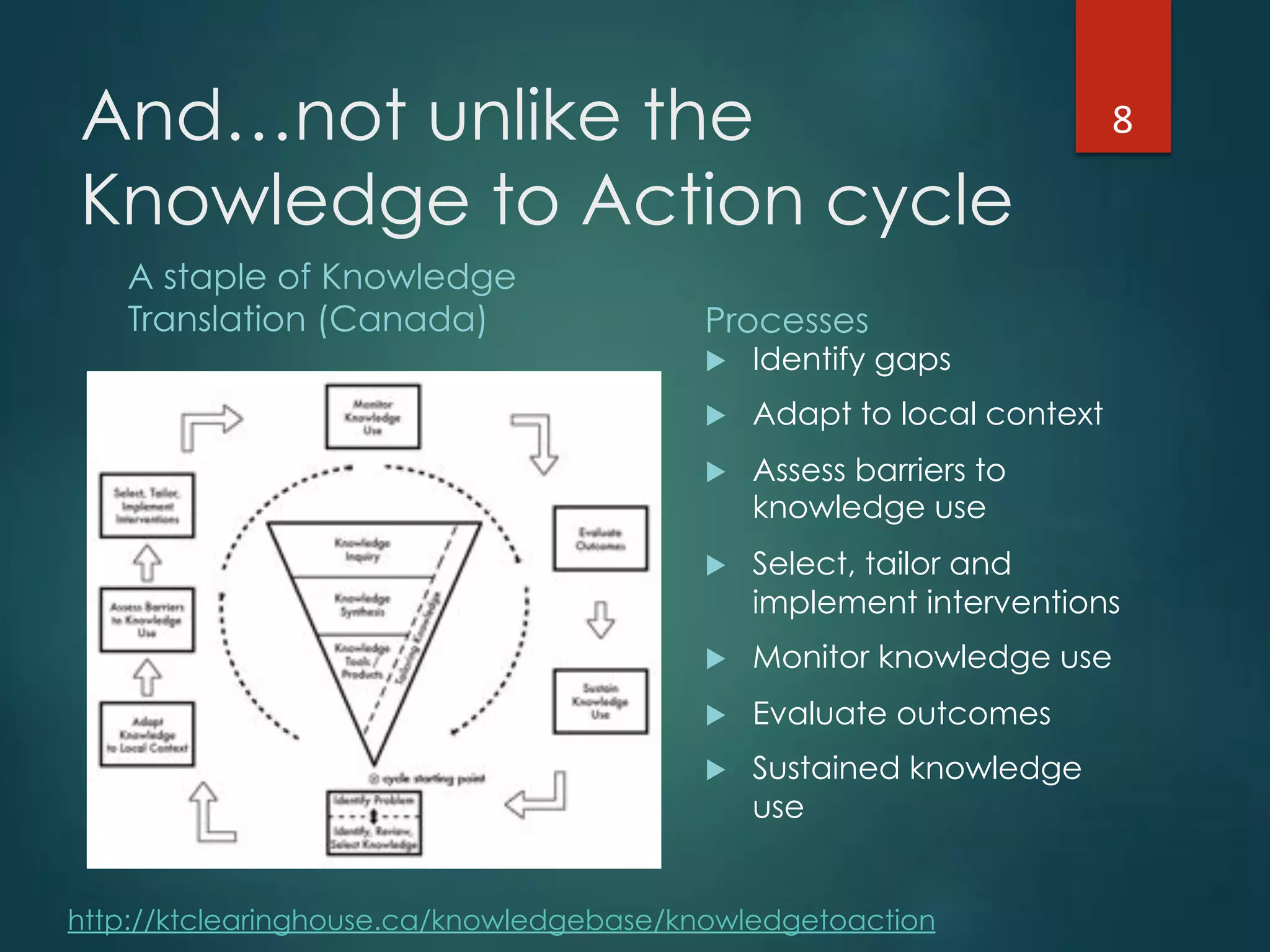

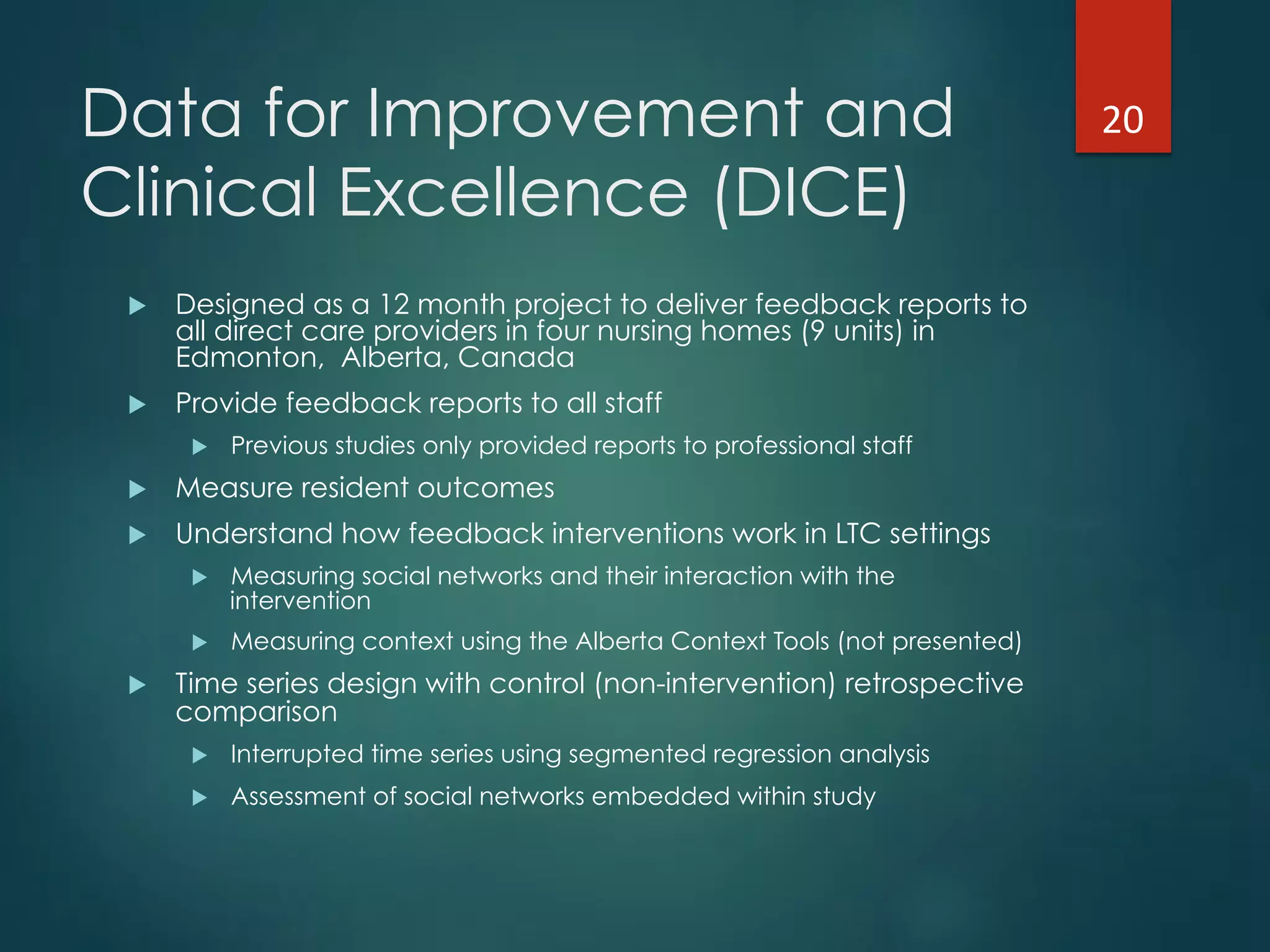

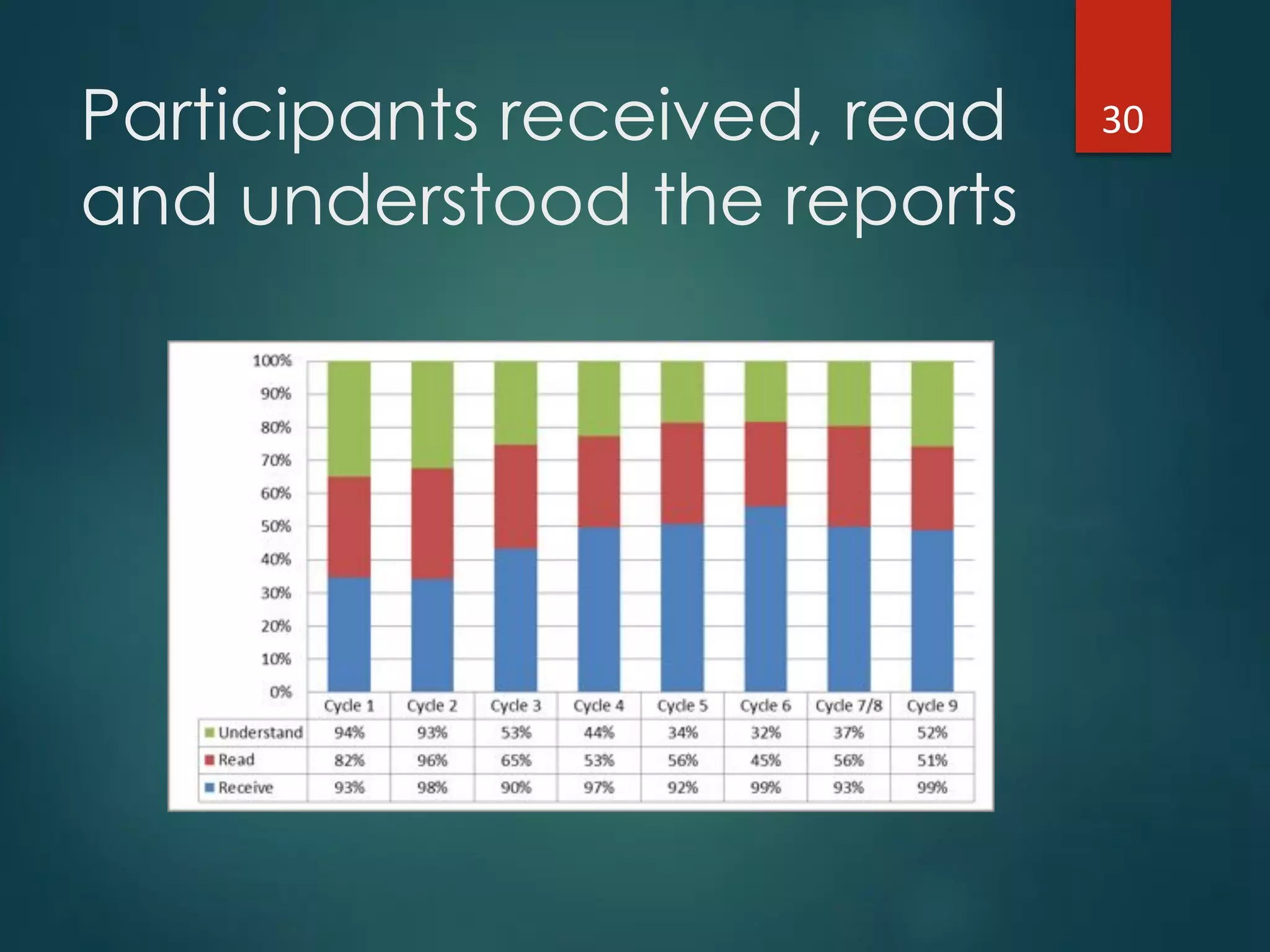
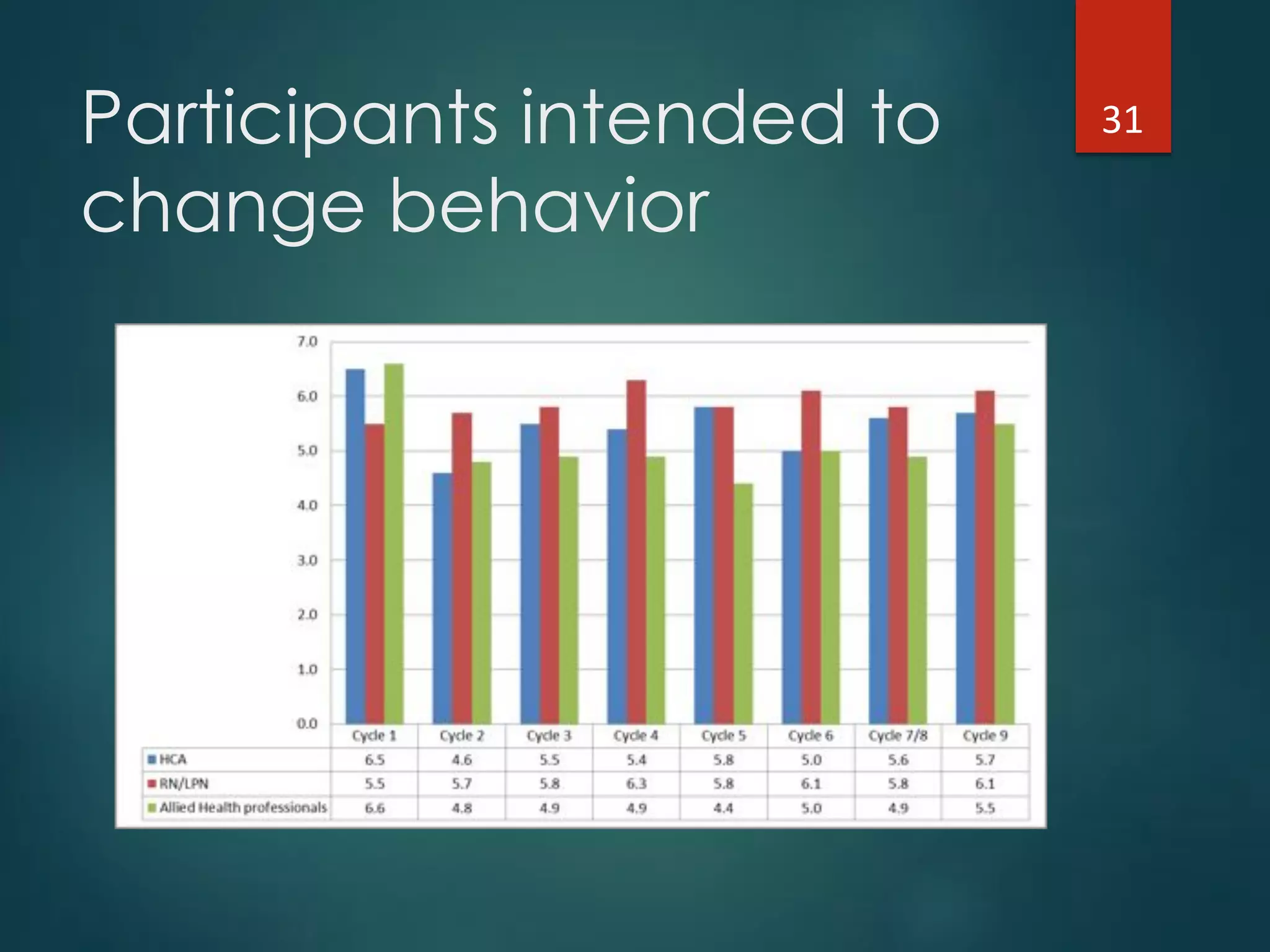
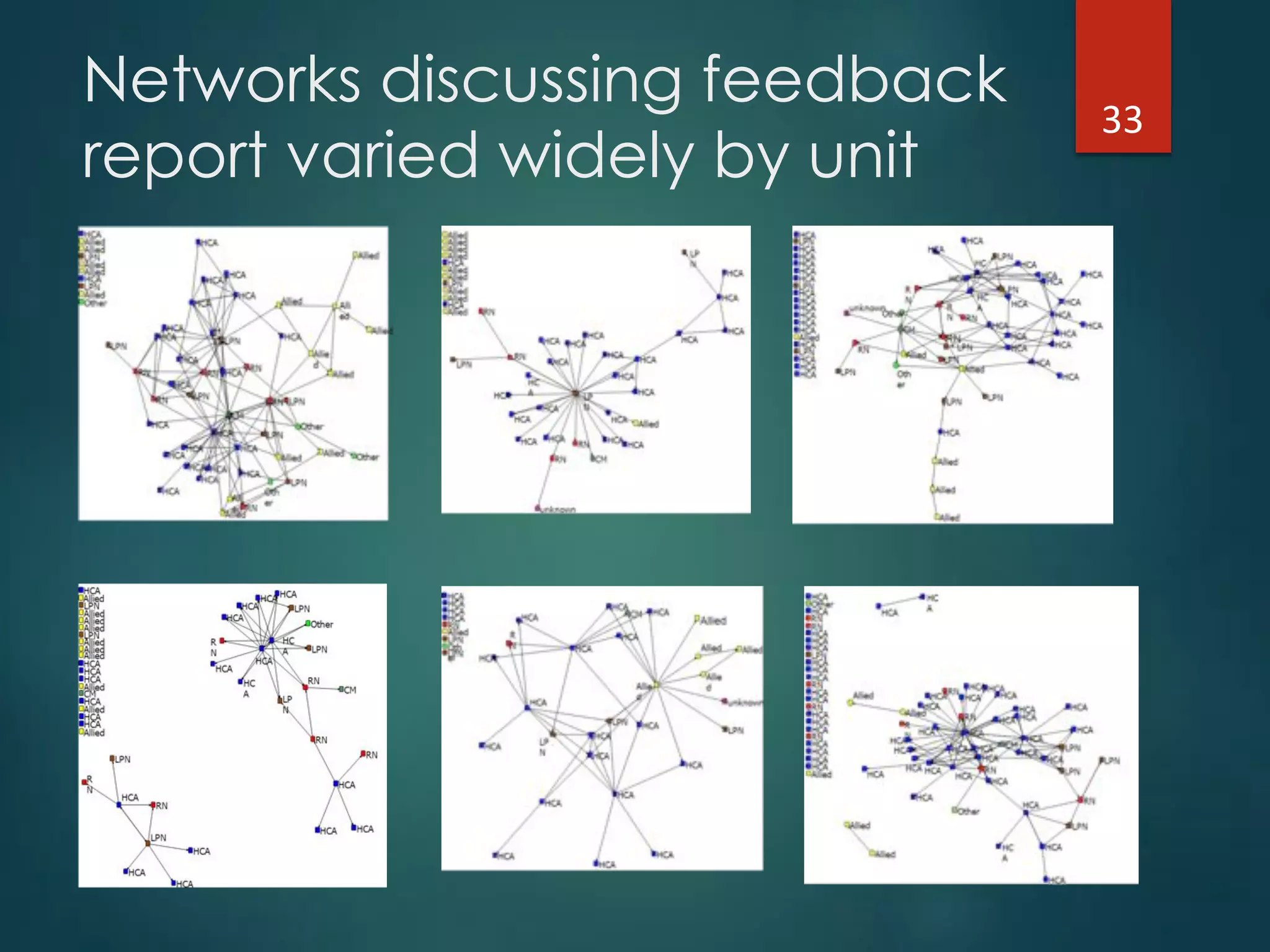
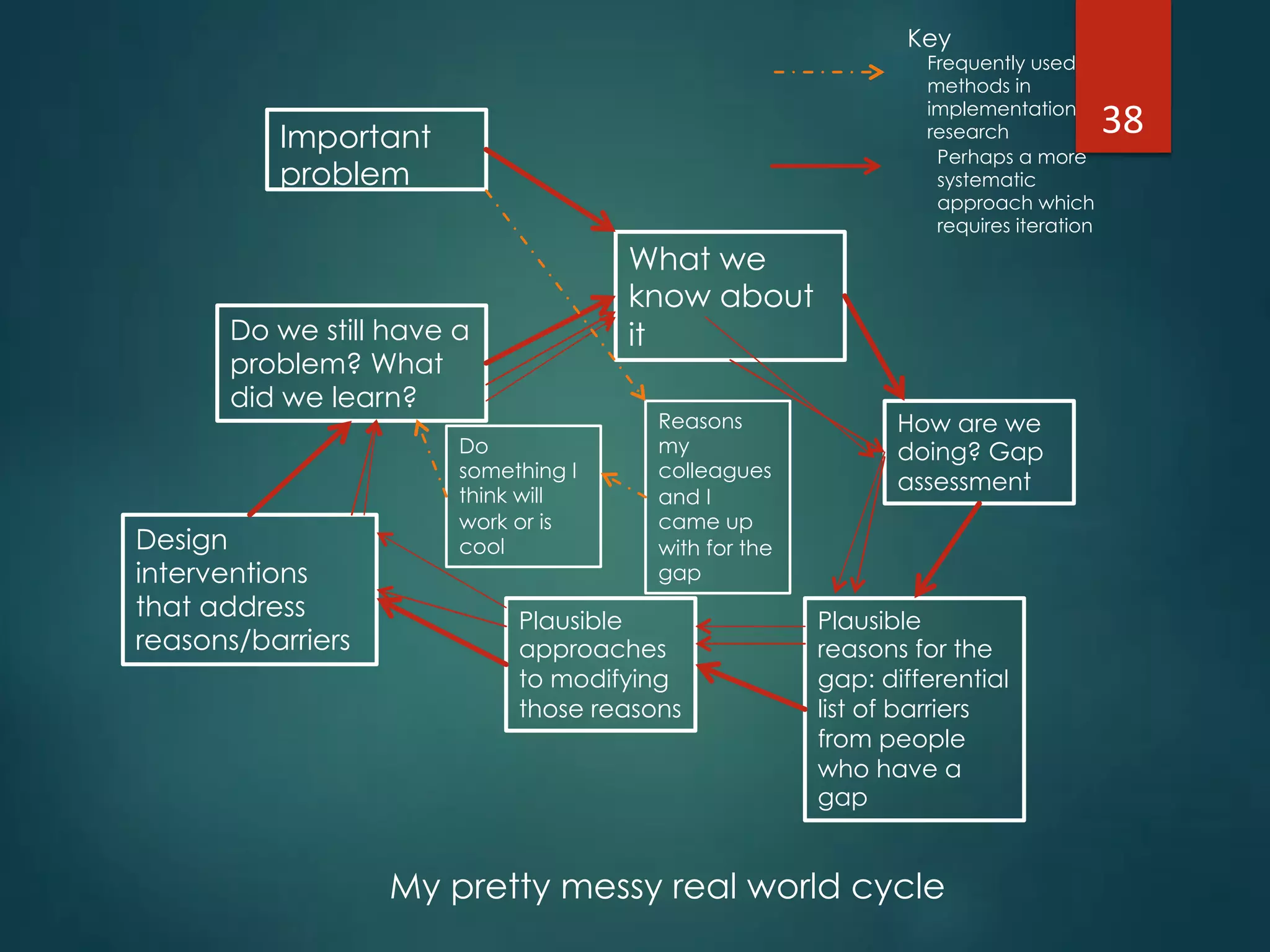
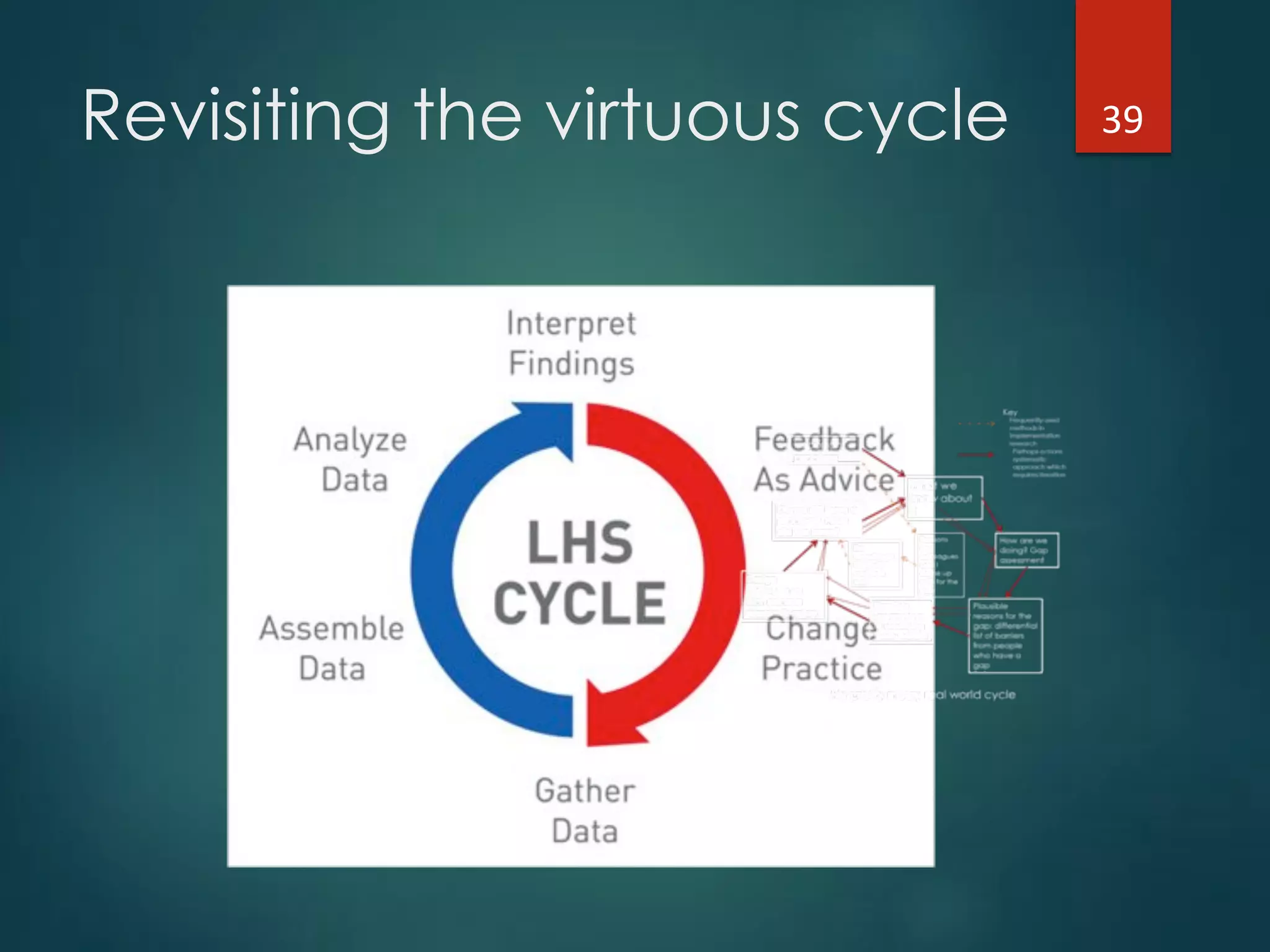
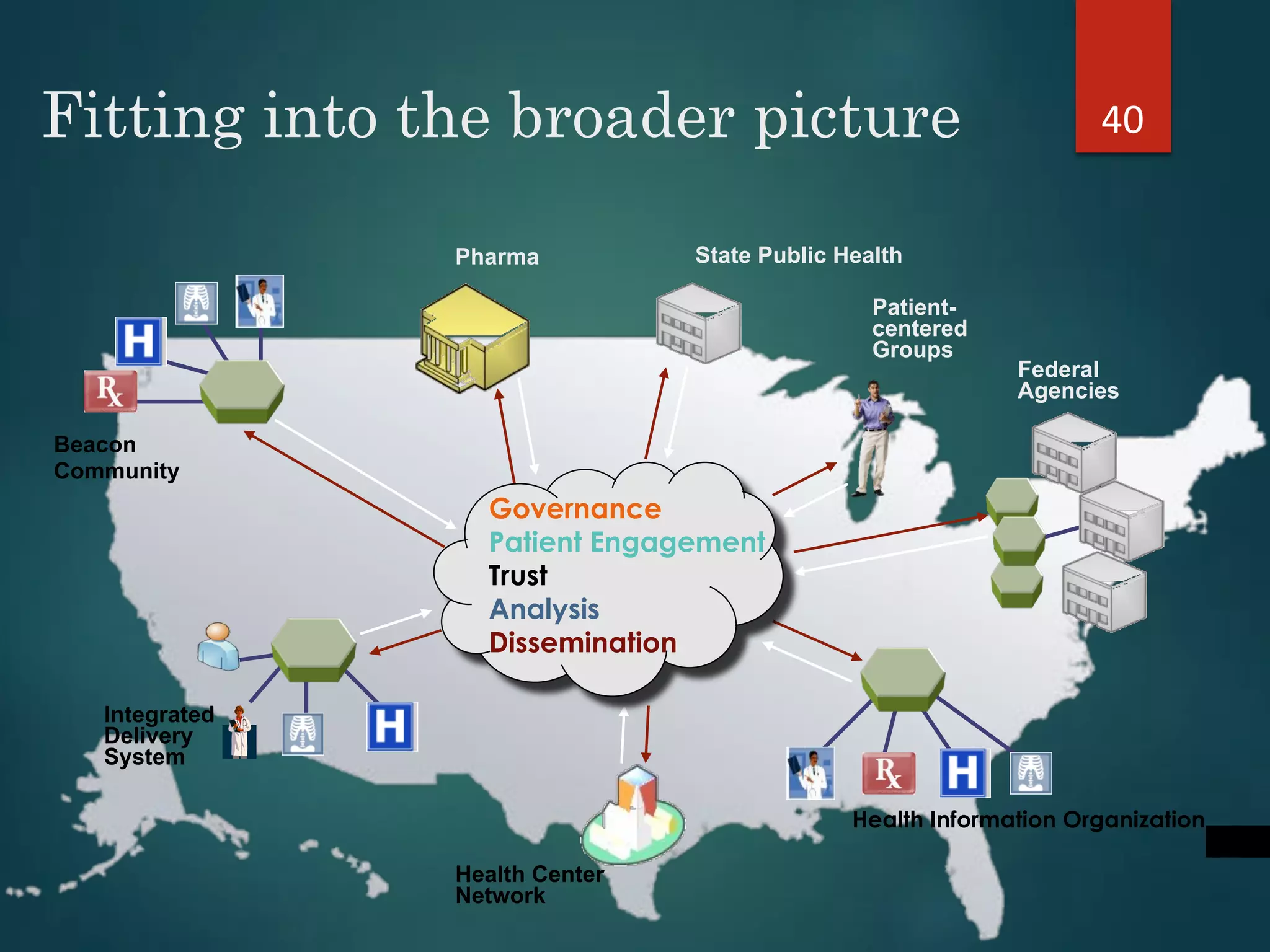
The document discusses the intersection of implementation science and learning health systems, highlighting their definitions, similarities, and differences. It describes the importance of evidence-based interventions in healthcare and provides an overview of recent research and frameworks in implementation science. Additionally, it presents a study on feedback interventions in long-term care settings, examining staff engagement and the impact on resident outcomes.