

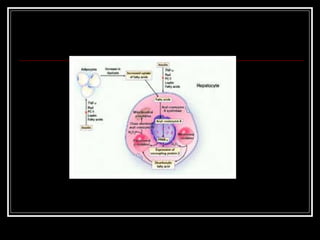



Non-alcoholic steatohepatitis (NASH) is a disease where fat accumulates in the liver in people who drink little or no alcohol. It is increasingly common in Western countries, especially in obese and diabetic patients. Insulin resistance and the accumulation of fat in the liver are thought to cause liver inflammation and damage. While many patients are asymptomatic, NASH can progress to cirrhosis in some cases over many years. Weight loss through diet and exercise is the best treatment option to reduce fat in the liver.









































































