Downloaded 150 times
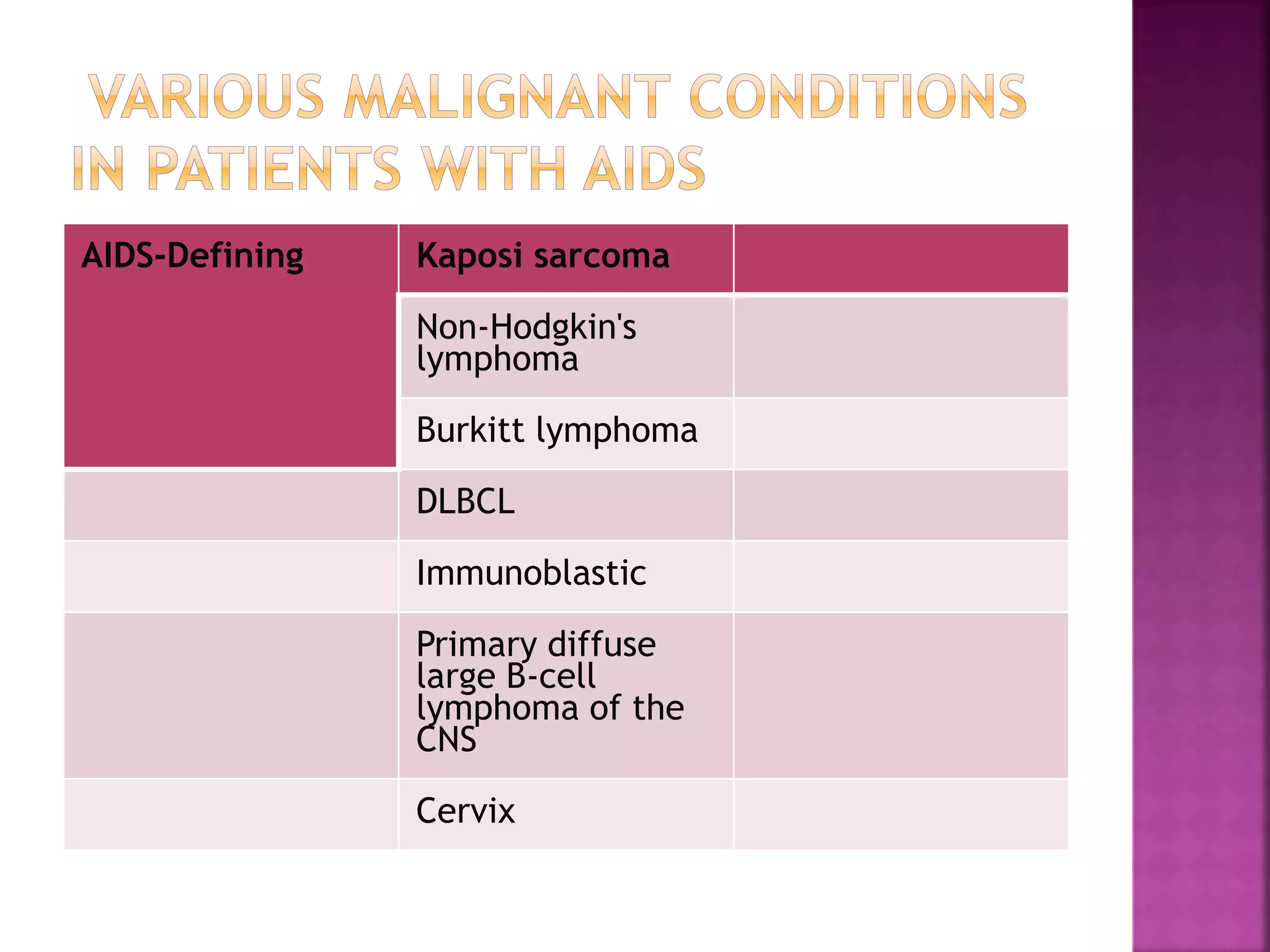
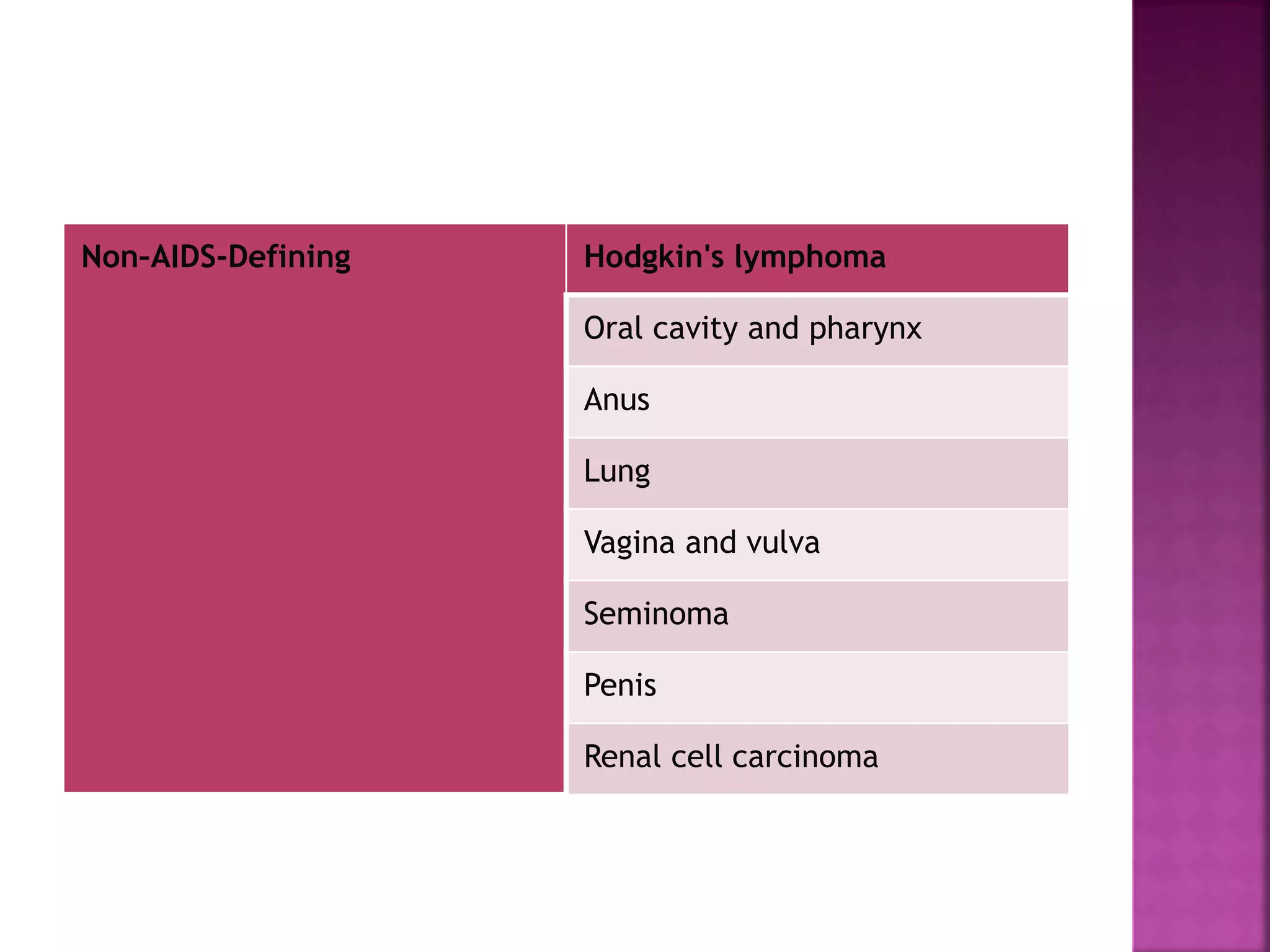
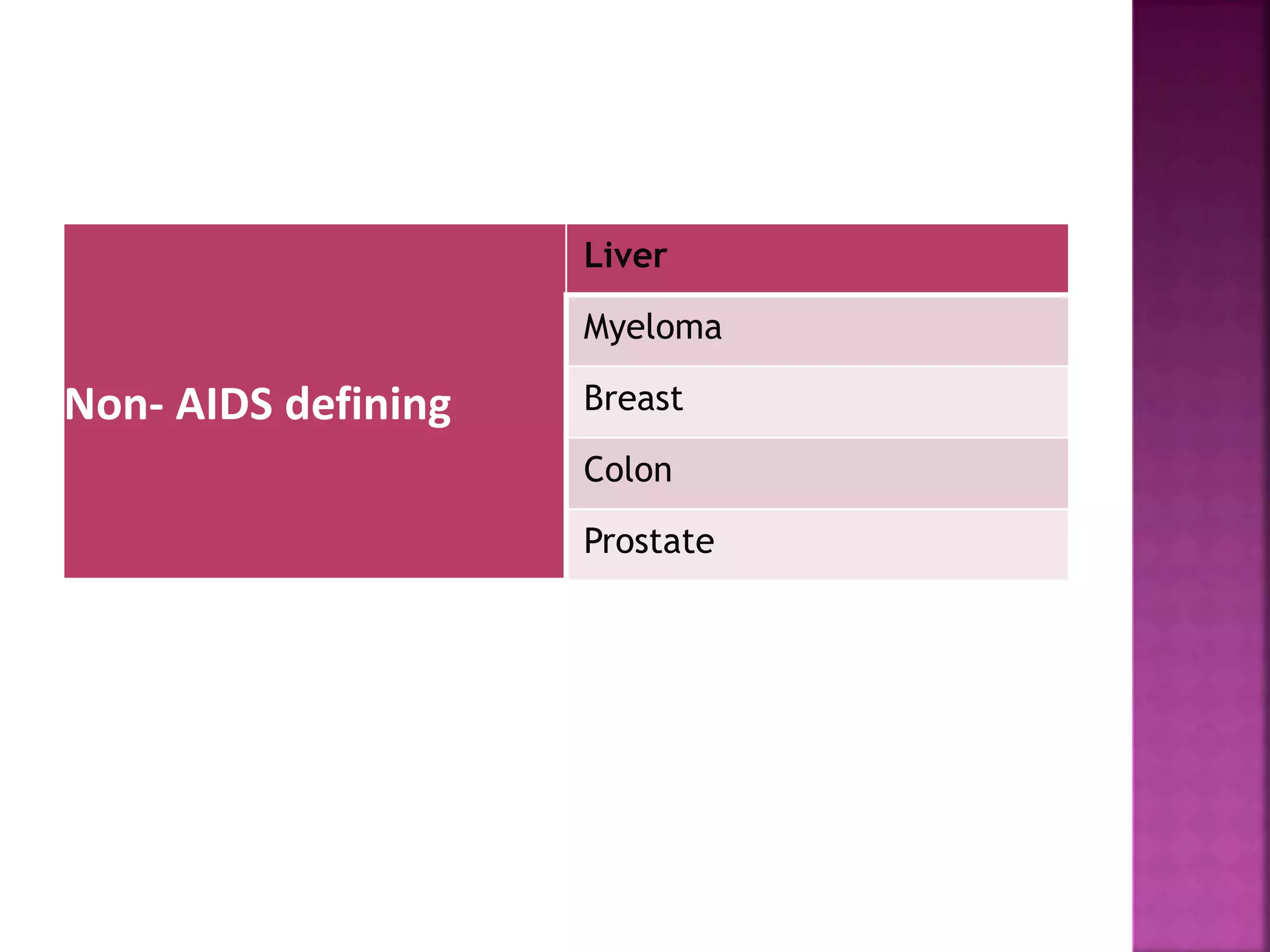
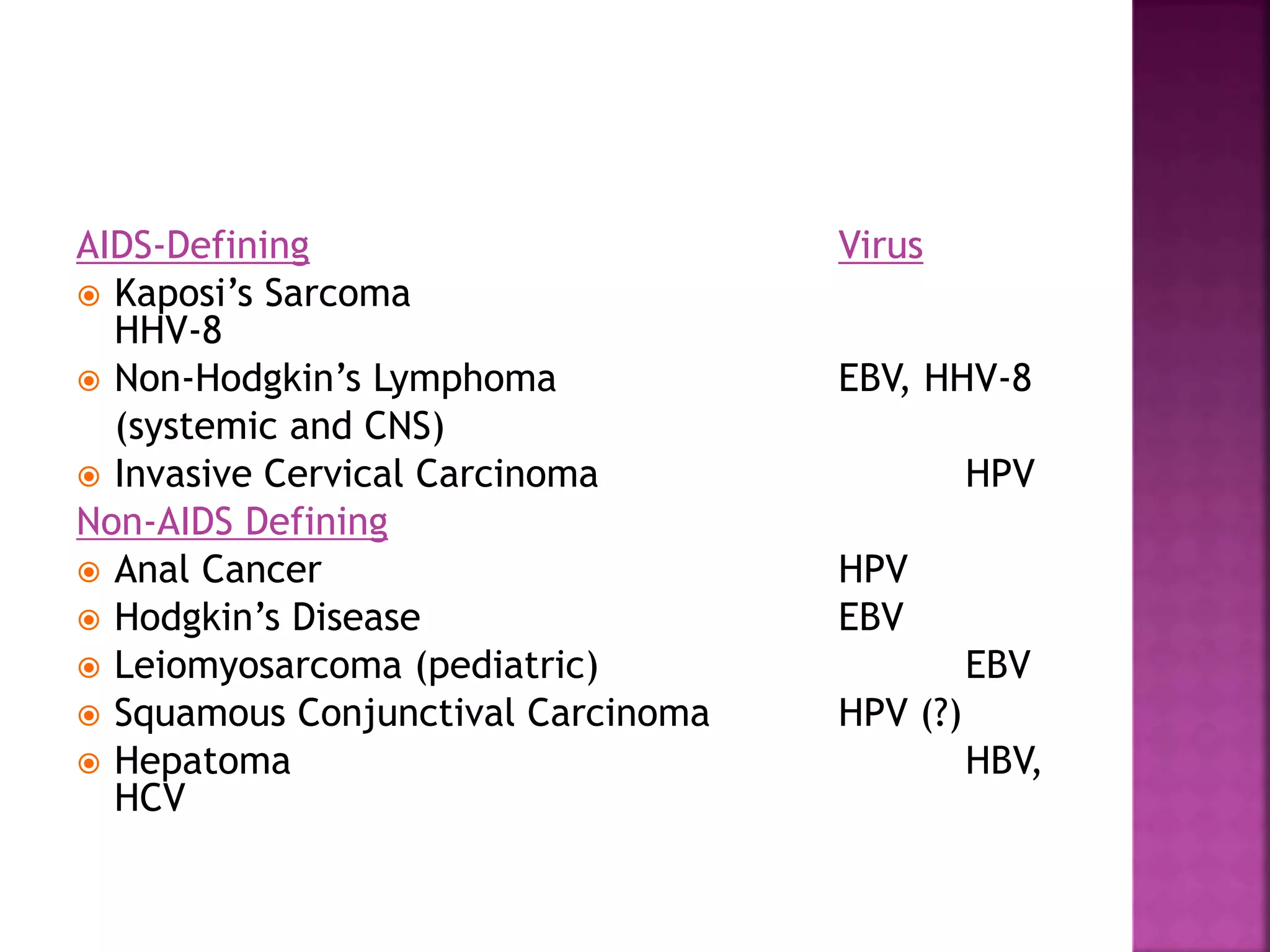



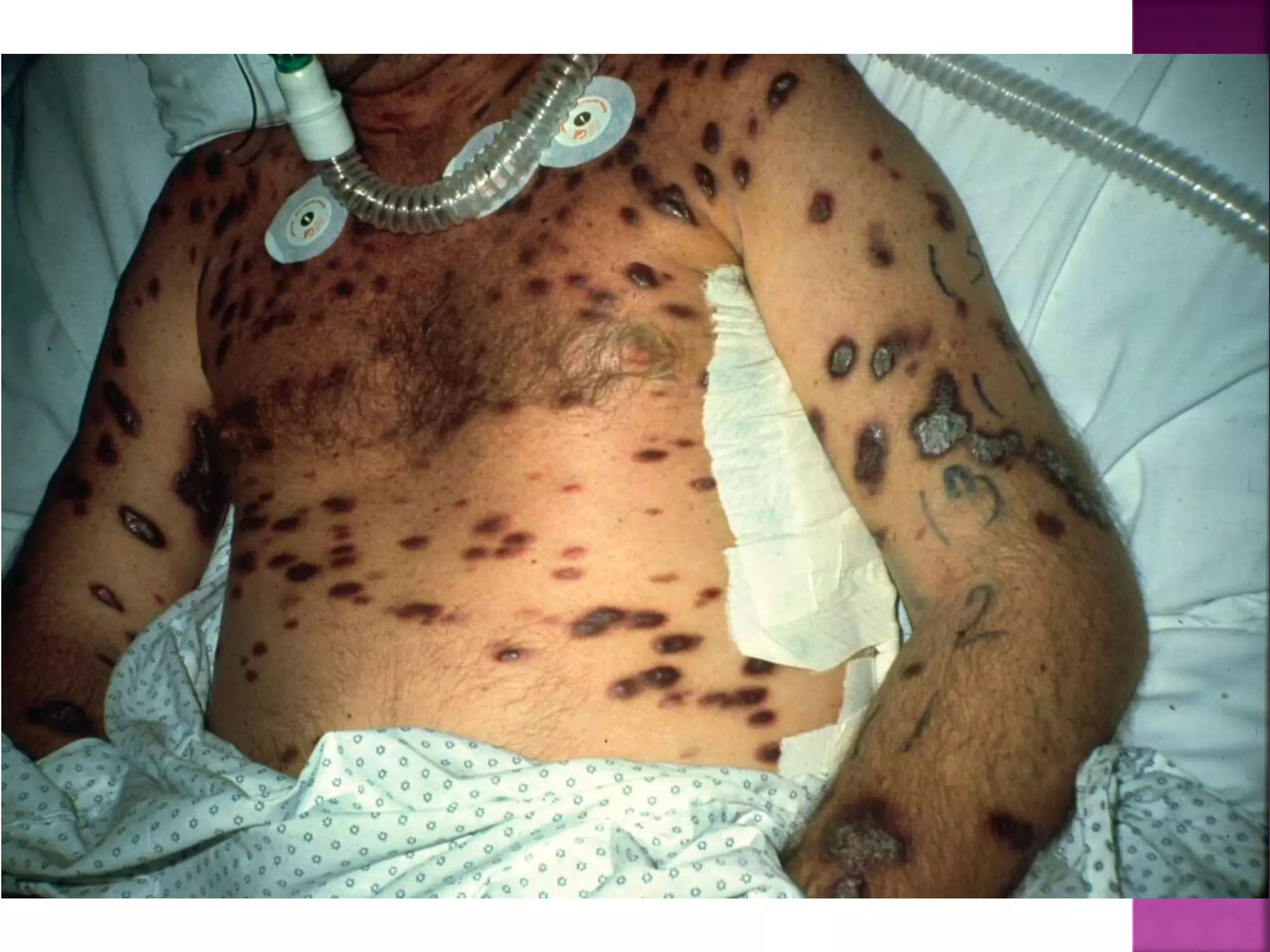



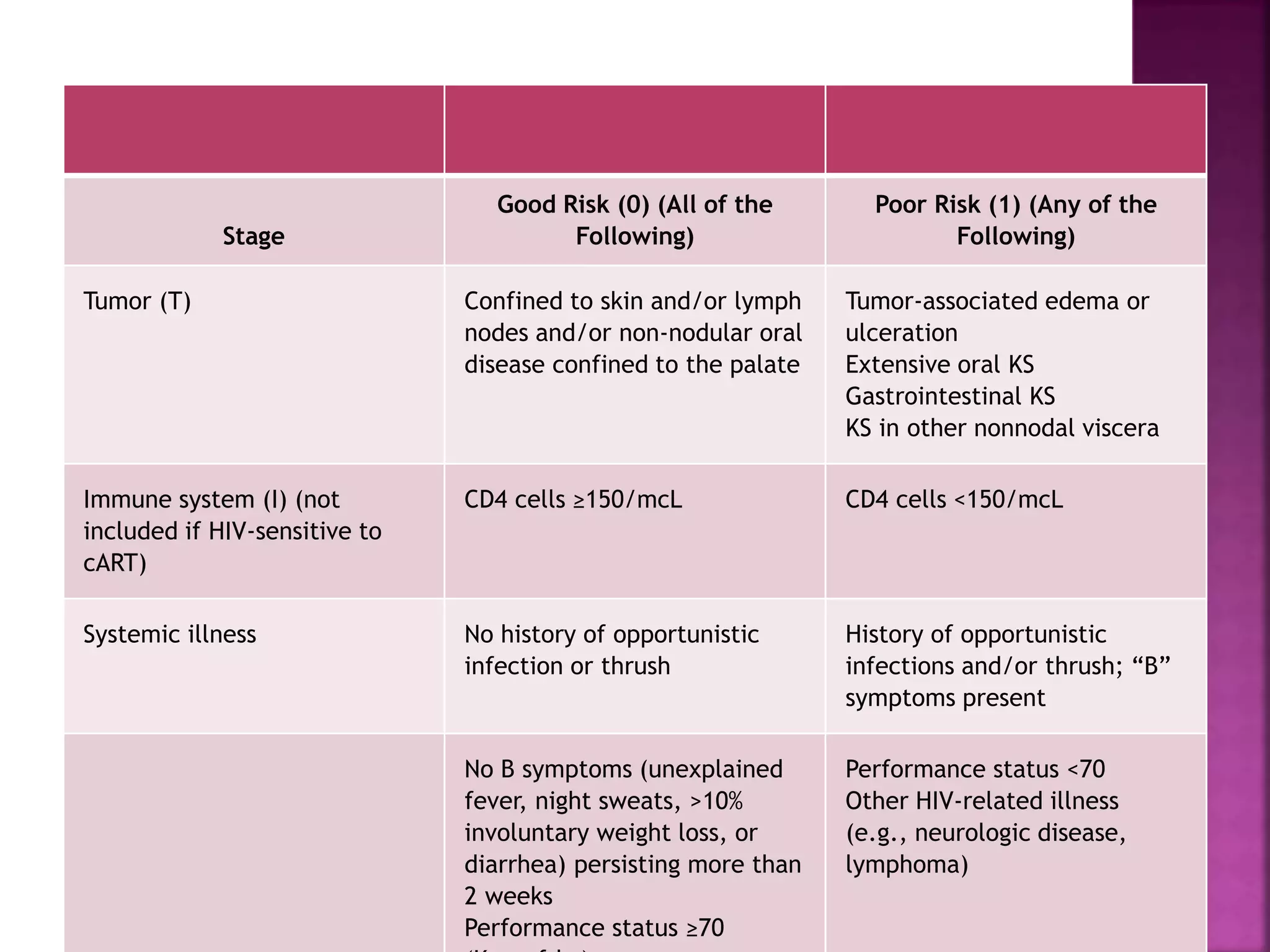
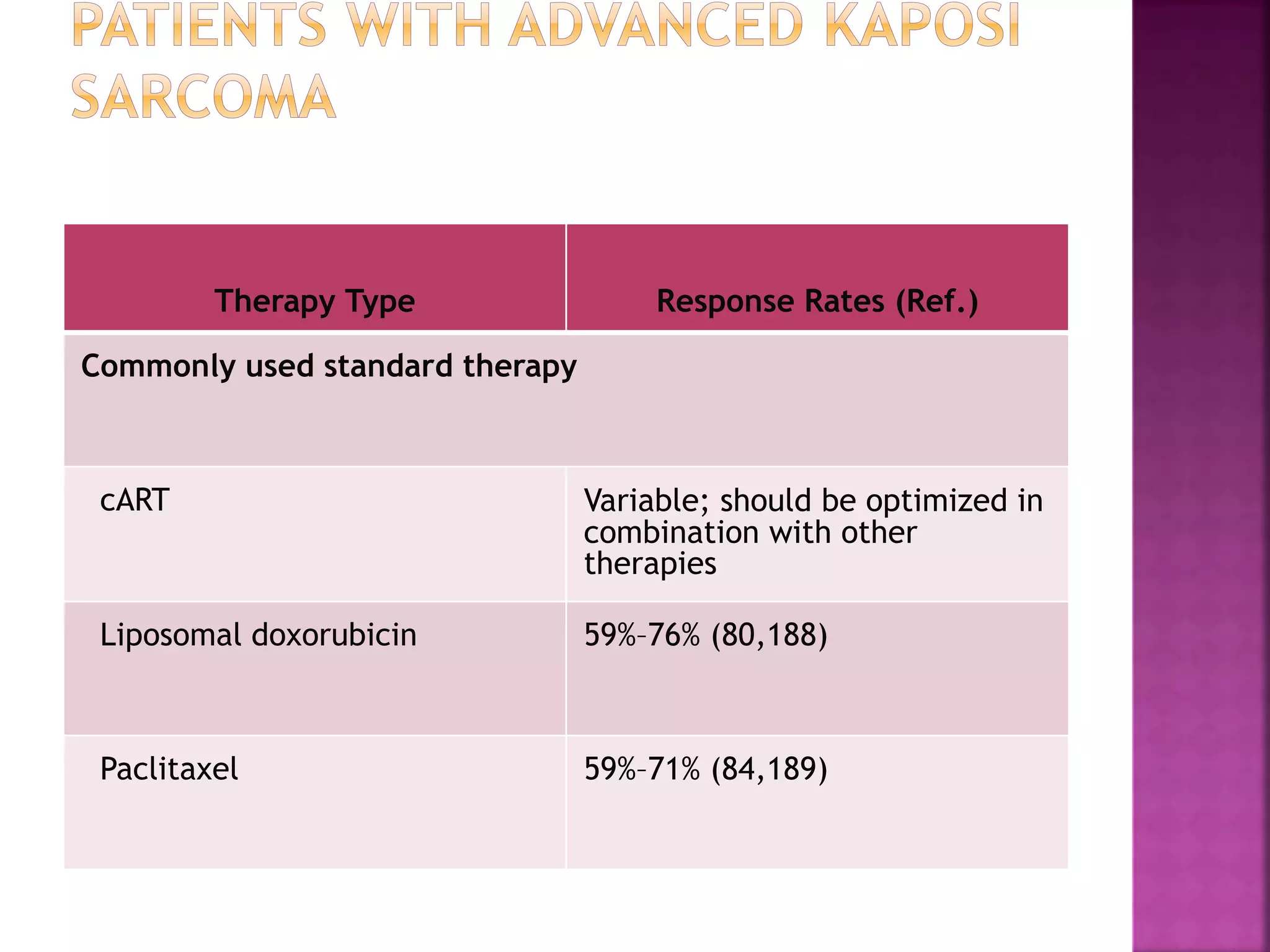

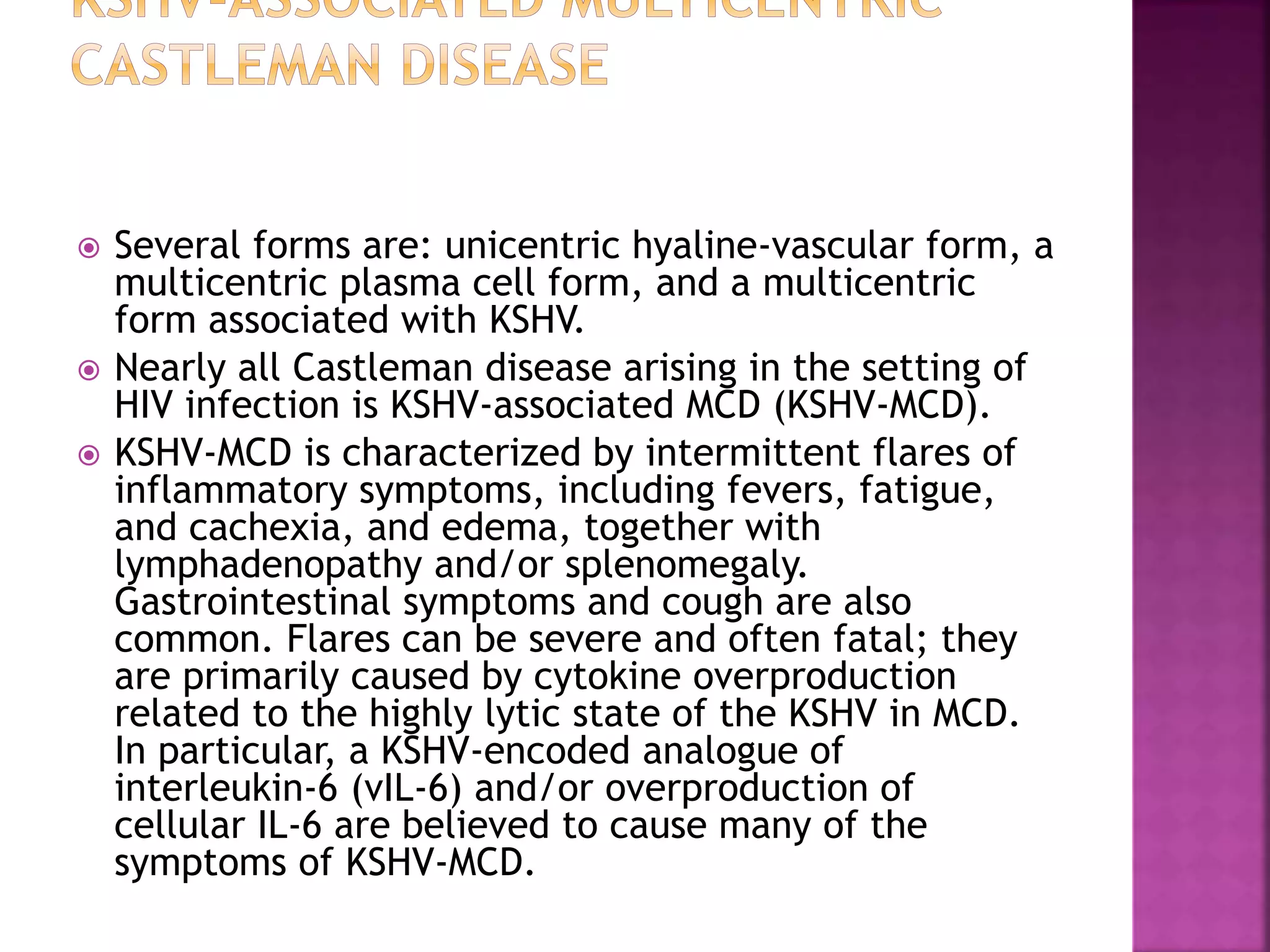
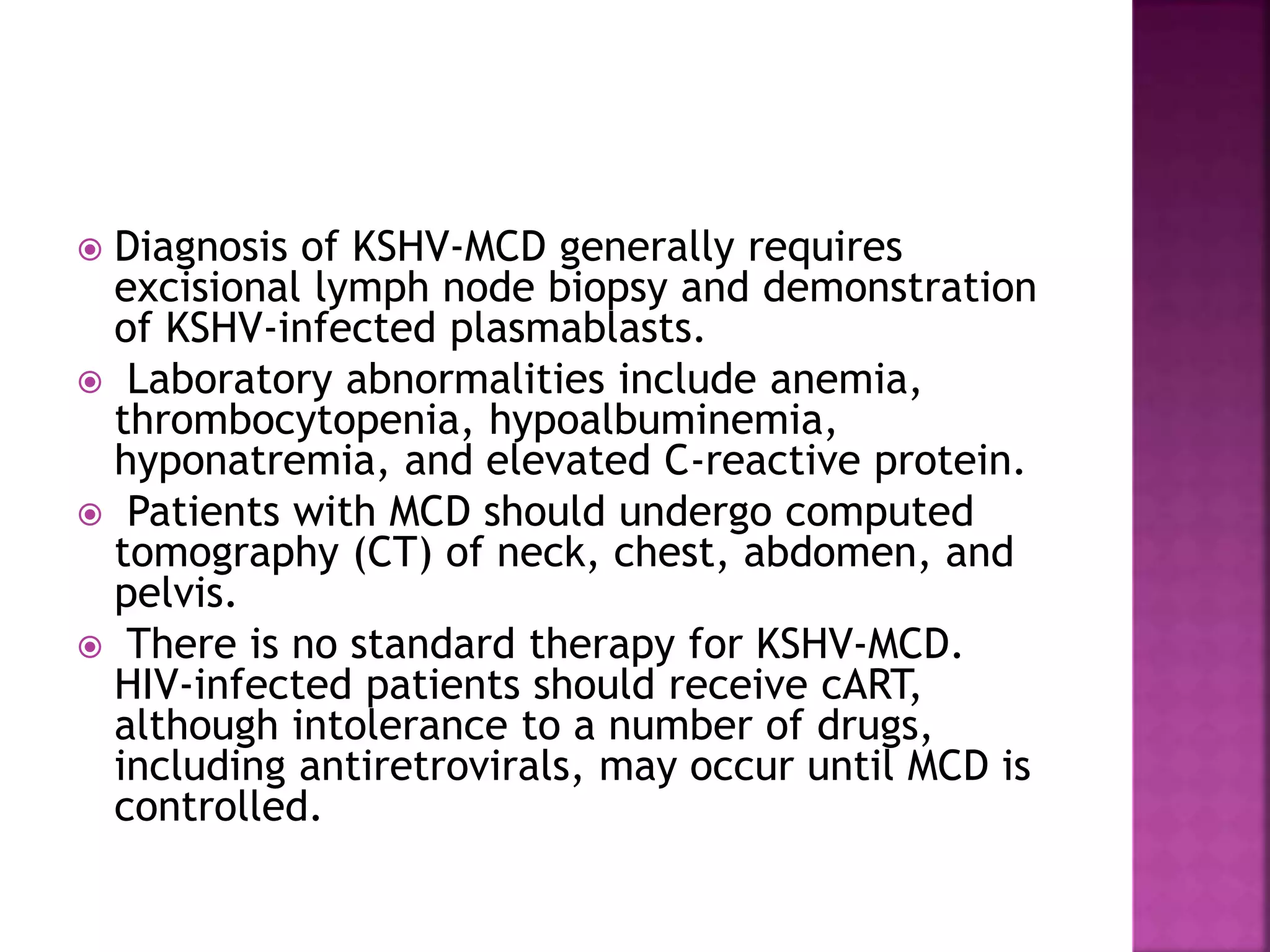














The document discusses several AIDS-defining and non-AIDS defining cancers that are more common in HIV-positive individuals. Kaposi sarcoma, caused by HHV-8, and two types of non-Hodgkin lymphoma were originally considered AIDS-defining cancers. While antiretroviral therapy has decreased AIDS deaths and increased the population of HIV-infected individuals, it has also led to an increase in both AIDS-defining and non-AIDS defining cancers due to people living longer with HIV. The document provides details on the pathogenesis, diagnosis and treatment of several AIDS-defining cancers including Kaposi sarcoma, multicentric Castleman's disease, and plasmablastic lymphoma.























































![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)































