Downloaded 71 times




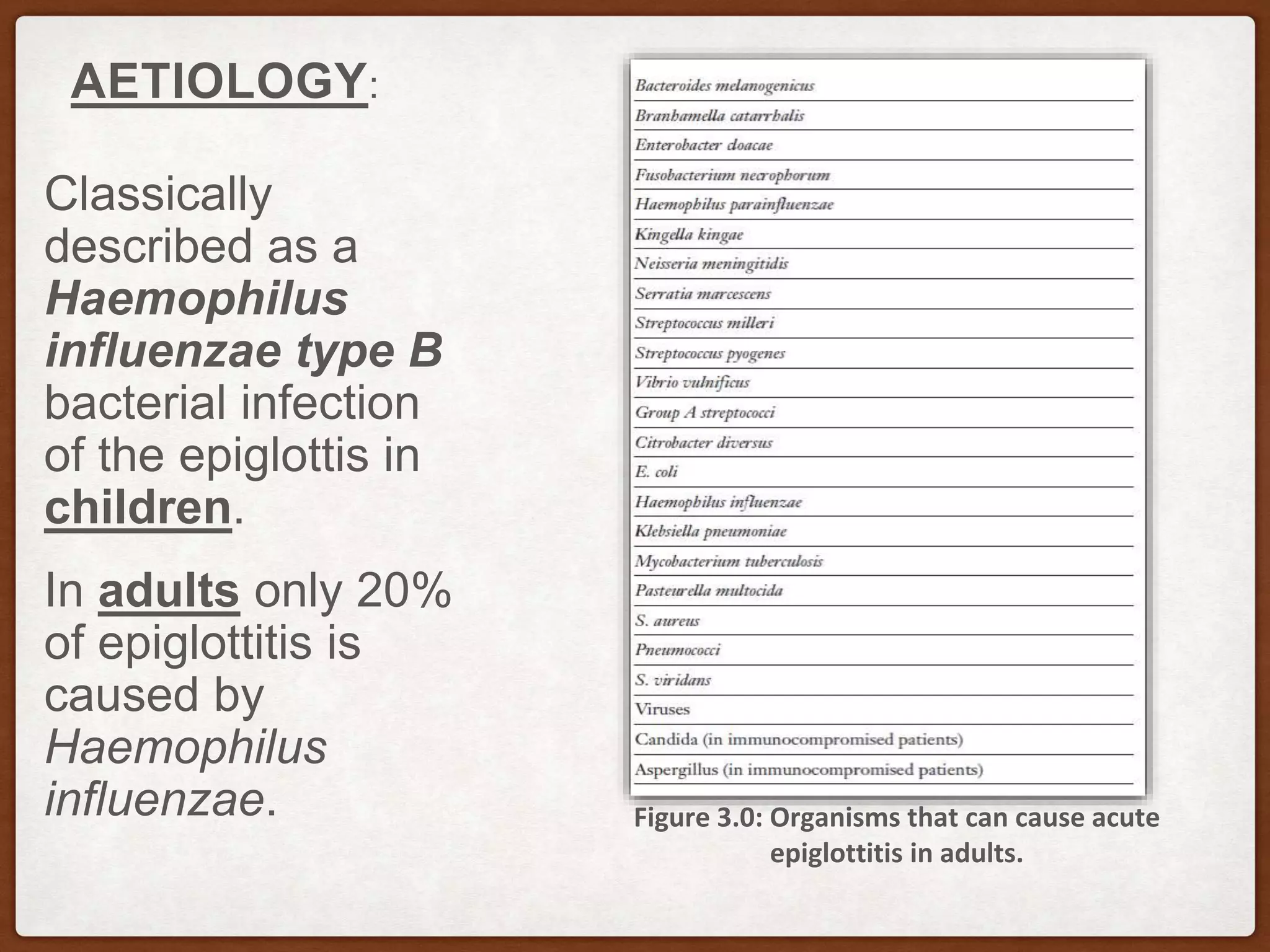


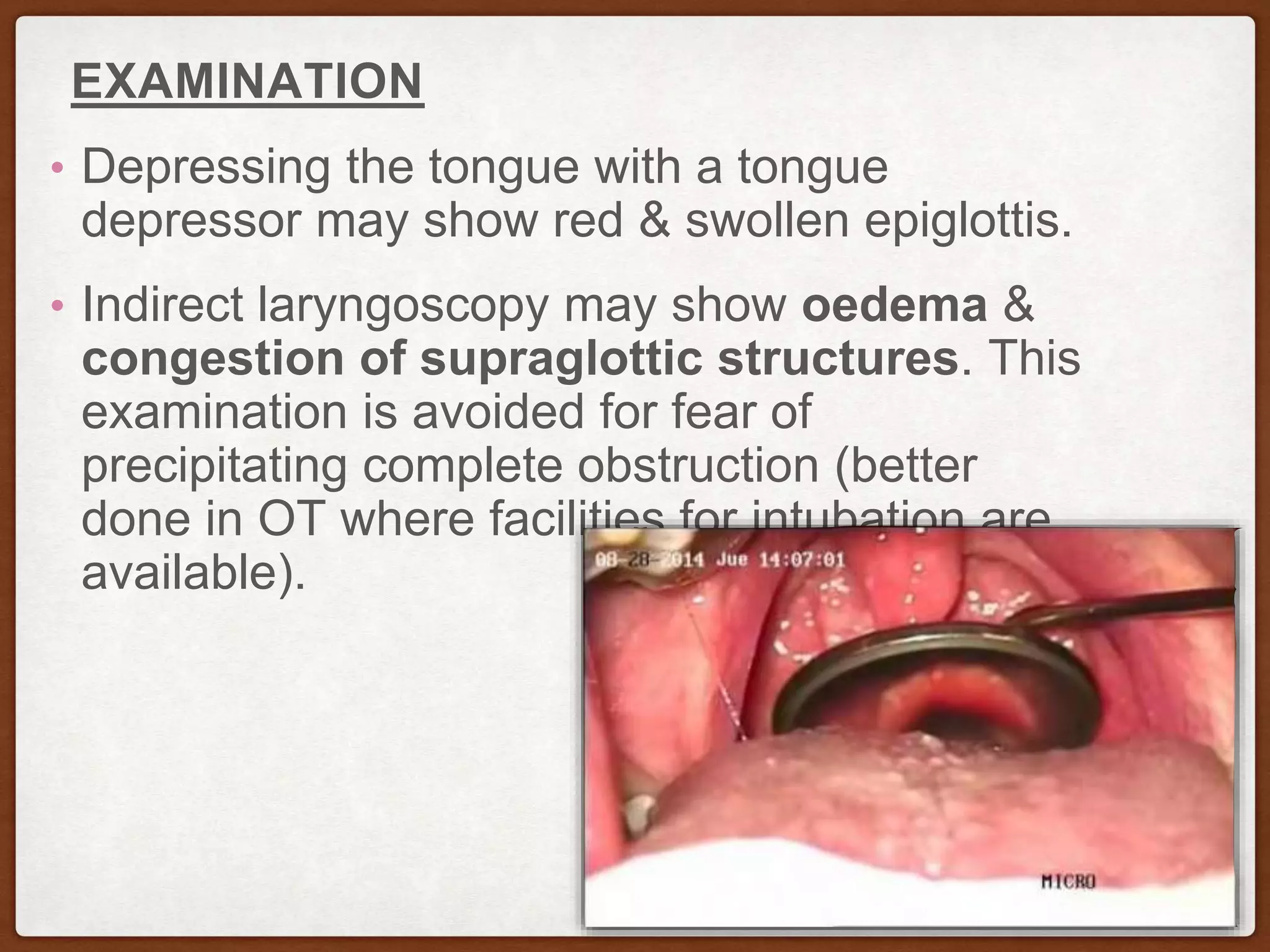






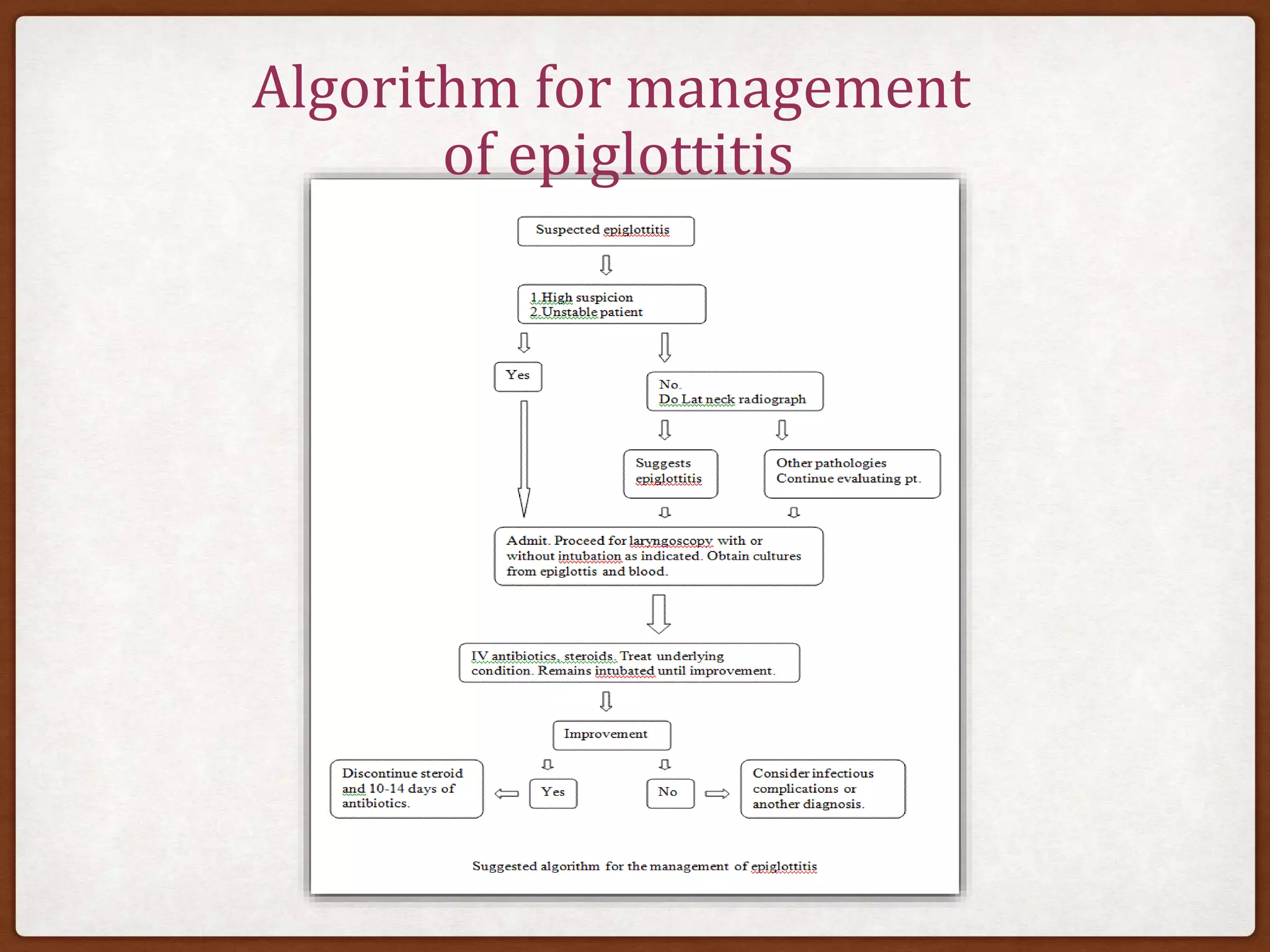




Acute epiglottitis is an inflammatory condition affecting supraglottic structures, often caused by infections such as Haemophilus influenzae type b, especially in children. Symptoms include severe sore throat, difficulty swallowing, and respiratory distress, with a risk of airway obstruction. Management requires hospitalization, use of antibiotics and steroids, and in severe cases, intubation or tracheostomy; while the prognosis is generally good with timely treatment, the risk of sudden airway compromise is significant.



































































