Downloaded 38 times
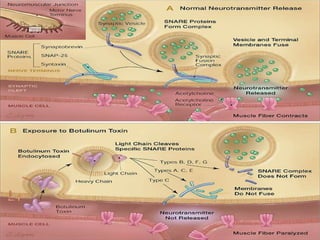
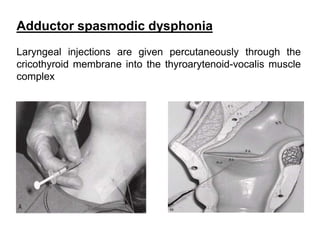
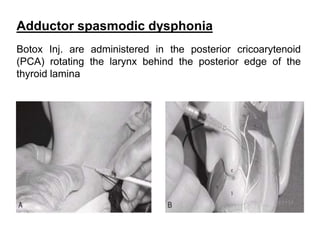



Botulinum toxin type A (Botox) and botulinum toxin type B are commonly used neuroparalytic agents to treat various ENT conditions like spasmodic dysphonia, oculopalatolaryngopharyngeal myoclonus, stuttering, and vocal tremors. Botox injections are administered to specific muscles to temporarily paralyze them. Potential adverse effects include pain, weakness, and dry mouth. Mitomycin C is an antiproliferative antibiotic used as a topical solution in ENT surgeries to decrease scar formation. Cidofovir is an antiviral medication approved to treat CMV retinitis but also used off-label for recurrent respiratory papillomat











































































