
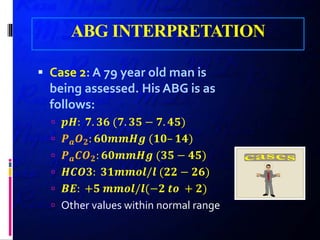
![ABG INTERPRETATION
Based on the iso-hydric
principle,
Acid: hydrogen-ion donor
Base: hydrogen-ion acceptor
Changes in [𝑯𝑯+
] alter virtually
all cellular function](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-29-320.jpg)
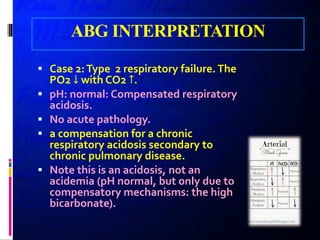
![ABG INTERPRETATION
the normal plasma [𝑯𝑯+
]:
very low 𝟒𝟒𝟒𝟒 𝒏𝒏𝒏𝒏𝒏𝒏𝒏𝒏/𝑳𝑳
the pH
−𝒍𝒍𝒍𝒍𝒍𝒍𝟏𝟏𝟏𝟏[𝑯𝑯+] = 𝒍𝒍𝒍𝒍𝒍𝒍𝟏𝟏𝟏𝟏
𝟏𝟏
[𝑯𝑯+]
is generally used in clinical medicine to
indicate acid–base status.
“acidemia”
Plasma pH is abnormally low (acidic)
“alkalemia”
Plasma pH is abnormally high (alkaline)](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-30-320.jpg)
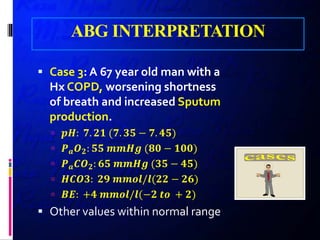
![ABG INTERPRETATION
the Henderson–Hasselbalch equation
𝒑𝒑𝒑𝒑 = 𝒑𝒑𝒑𝒑 + 𝒍𝒍𝒍𝒍𝒍𝒍𝟏𝟏𝟏𝟏(
𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−
𝟎𝟎. 𝟎𝟎𝟎𝟎 × 𝑷𝑷𝒂𝒂 𝑪𝑪𝑶𝑶𝟐𝟐
)
𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−
= proton acceptor = BASE (KIDNEY)
𝑪𝑪𝑪𝑪𝟐𝟐 = proton donor = ACID (LUNG)
𝒑𝒑𝒑𝒑 = 𝒑𝒑𝒑𝒑 + 𝒍𝒍𝒍𝒍𝒍𝒍𝟏𝟏𝟏𝟏([𝑩𝑩𝑩𝑩𝑩𝑩𝑩𝑩] / [𝑨𝑨𝑨𝑨𝑨𝑨𝑨𝑨])
𝒑𝒑𝒑𝒑 = 𝒑𝒑𝒑𝒑 + 𝒍𝒍𝒍𝒍𝒍𝒍𝟏𝟏𝟏𝟏([𝒌𝒌𝒌𝒌𝒌𝒌𝒌𝒌𝒌𝒌𝒌𝒌] / [𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍])](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-32-320.jpg)
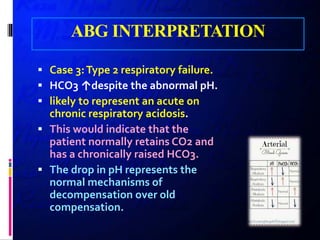
![ABG INTERPRETATION
pH = pK + log10 ([kidney] / [lung])
ACIDOSIS:
Respiratory
Metabolic
ALKALOSIS:
Respiratory
Metabolic](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-34-320.jpg)
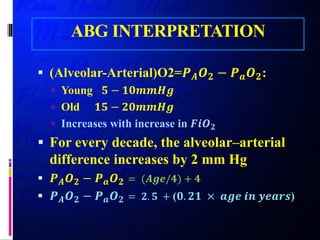
![ABG INTERPRETATION
Metabolic acidosis
𝒑𝒑𝒑𝒑 < 𝟕𝟕. 𝟑𝟑𝟑𝟑 and [𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−
] < 𝟐𝟐𝟐𝟐 𝒎𝒎𝒎𝒎𝒎𝒎𝒎𝒎/𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍
𝑩𝑩𝑩𝑩 < −𝟐𝟐 𝒎𝒎𝒎𝒎𝒎𝒎𝒎𝒎/𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍
Secondary (respiratory) response:
𝑷𝑷𝒂𝒂 𝑪𝑪𝑶𝑶𝟐𝟐 = 𝟏𝟏. 𝟓𝟓 × [𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−] + 𝟖𝟖 ± 𝟐𝟐 𝒎𝒎𝒎𝒎 𝑯𝑯𝑯𝑯
or
𝑷𝑷𝒂𝒂 𝑪𝑪𝑶𝑶𝟐𝟐 = [𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−] + 𝟏𝟏𝟏𝟏 𝒎𝒎𝒎𝒎 𝑯𝑯𝑯𝑯
Complete secondary adaptive response within 12–24 hr](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-35-320.jpg)
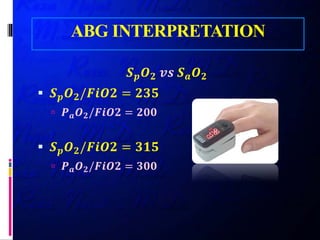
![ABG INTERPRETATION
Metabolic alkalosis
𝒑𝒑𝒑𝒑 > 𝟕𝟕. 𝟒𝟒𝟒𝟒 and [𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−] > 𝟐𝟐𝟐𝟐 𝒎𝒎𝒎𝒎𝒎𝒎𝒎𝒎/𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍
𝑩𝑩𝑩𝑩 > +𝟐𝟐 𝒎𝒎𝒎𝒎𝒎𝒎𝒎𝒎/𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍
Secondary (respiratory) response:
𝑷𝑷𝒂𝒂 𝑪𝑪𝑶𝑶𝟐𝟐 = 𝟎𝟎. 𝟕𝟕 × ([𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−] − 𝟐𝟐𝟐𝟐) + 𝟒𝟒𝟒𝟒 ± 𝟐𝟐 𝒎𝒎𝒎𝒎 𝑯𝑯𝑯𝑯
or
𝑷𝑷𝒂𝒂 𝑪𝑪𝑶𝑶𝟐𝟐 = [𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−
] + 𝟏𝟏𝟏𝟏 𝒎𝒎𝒎𝒎 𝑯𝑯𝑯𝑯
or
𝑷𝑷𝒂𝒂 𝑪𝑪𝑶𝑶𝟐𝟐 = 𝟎𝟎. 𝟕𝟕 × [𝑯𝑯𝑯𝑯𝑯𝑯𝑯𝑯−
] + 𝟐𝟐𝟐𝟐 𝒎𝒎𝒎𝒎 𝑯𝑯𝑯𝑯
Complete secondary adaptive response within 24–36 hr](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-36-320.jpg)
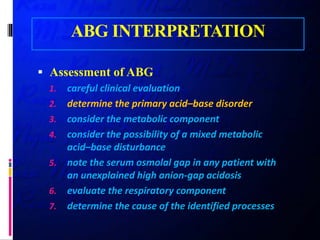
![ABG INTERPRETATION
Calculation of the anion gap:
[𝑵𝑵𝑵𝑵+
] + [𝑲𝑲+
] + [𝑪𝑪𝑪𝑪𝟐𝟐+
] + [𝑴𝑴𝑴𝑴𝟐𝟐+
] + + [𝑯𝑯+
]
+ 𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖 𝒄𝒄𝒄𝒄𝒄𝒄𝒄𝒄𝒄𝒄𝒄𝒄𝒄𝒄 = [𝑪𝑪𝑪𝑪−
] + [𝑯𝑯𝑪𝑪𝑪𝑪𝟑𝟑
−
]
+ [𝑪𝑪𝑪𝑪𝟑𝟑
𝟐𝟐−
] + [𝑶𝑶𝑶𝑶−
] + 𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂
+ 𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑𝒑 + 𝒔𝒔𝒔𝒔𝒔𝒔𝒔𝒔𝒔𝒔𝒔𝒔𝒔𝒔 + 𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍𝒍
+ 𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖𝒖 𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂𝒂
𝑨𝑨𝑨𝑨𝑨𝑨𝑨𝑨𝑨𝑨 𝑮𝑮𝑮𝑮𝑮𝑮 = [𝑵𝑵𝑵𝑵+
] − ([𝑪𝑪𝑪𝑪−
] + [𝑯𝑯𝑪𝑪𝑪𝑪𝟑𝟑
−
])
= 𝑼𝑼𝑼𝑼 − 𝑼𝑼𝑼𝑼
= 𝟏𝟏𝟏𝟏 − 𝟏𝟏𝟏𝟏𝟏𝟏𝟏𝟏𝟏𝟏/𝑳𝑳](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-41-320.jpg)
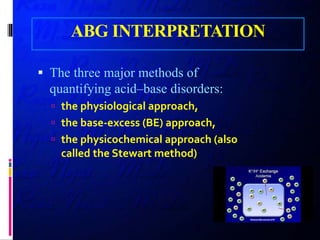
![ABG INTERPRETATION
High anion-gap metabolic acidosis
GOLD MARRK
Glycols [ethylene and propylene],
5-oxoproline [pyroglutamic acid],
l-lactate,
d-lactate,
methanol,
aspirin,
renal failure,
rhabdomyolysis,
ketoacidosis](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-43-320.jpg)
![ABG INTERPRETATION
Normal Anion Gap Acidosis:
GI or Urinary HCO3- loss
Urinary Anion GAP:
( 𝑵𝑵𝑵𝑵+
+ 𝑲𝑲+
)– [𝑪𝑪𝑪𝑪−
]
neGUTive GI (diarrhea), PRTA
Positive in RF, DRTA, Hypoaldosteronism](https://image.slidesharecdn.com/acidbaseheartcongress96final-181217194938/85/Acid-base-heart-congress-96-final-44-320.jpg)
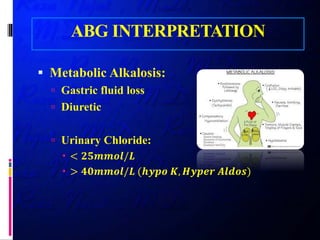

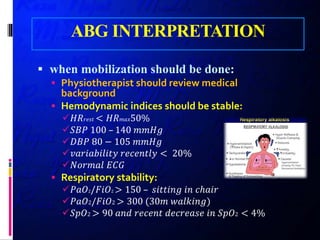
The document discusses the importance of ABG (arterial blood gas) interpretation and physiotherapy recommendations for critically ill patients, particularly in the ICU. It emphasizes the necessity of careful monitoring and intervention strategies to enhance respiratory function, decrease length of stay, and improve patient outcomes. Key considerations include assessing hemodynamic status, the impact of positioning, and understanding metabolic and respiratory acid-base disorders.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







