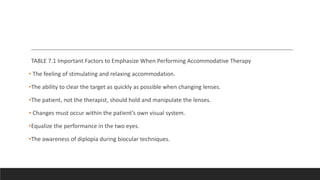
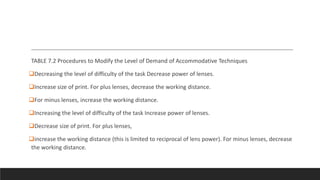
The document outlines accommodative vision therapy, which aims to improve accommodative amplitude and facility through various techniques and equipment, including plus and minus lenses. It describes specific procedures like the Red-Red Rock anaglyphic method and computer programs that utilize liquid crystal glasses, focusing on patient engagement and gradual increases in difficulty. Key endpoints for therapy are provided according to the patient's age and accommodative ability, emphasizing the development of awareness and control over accommodation.





























![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)























































