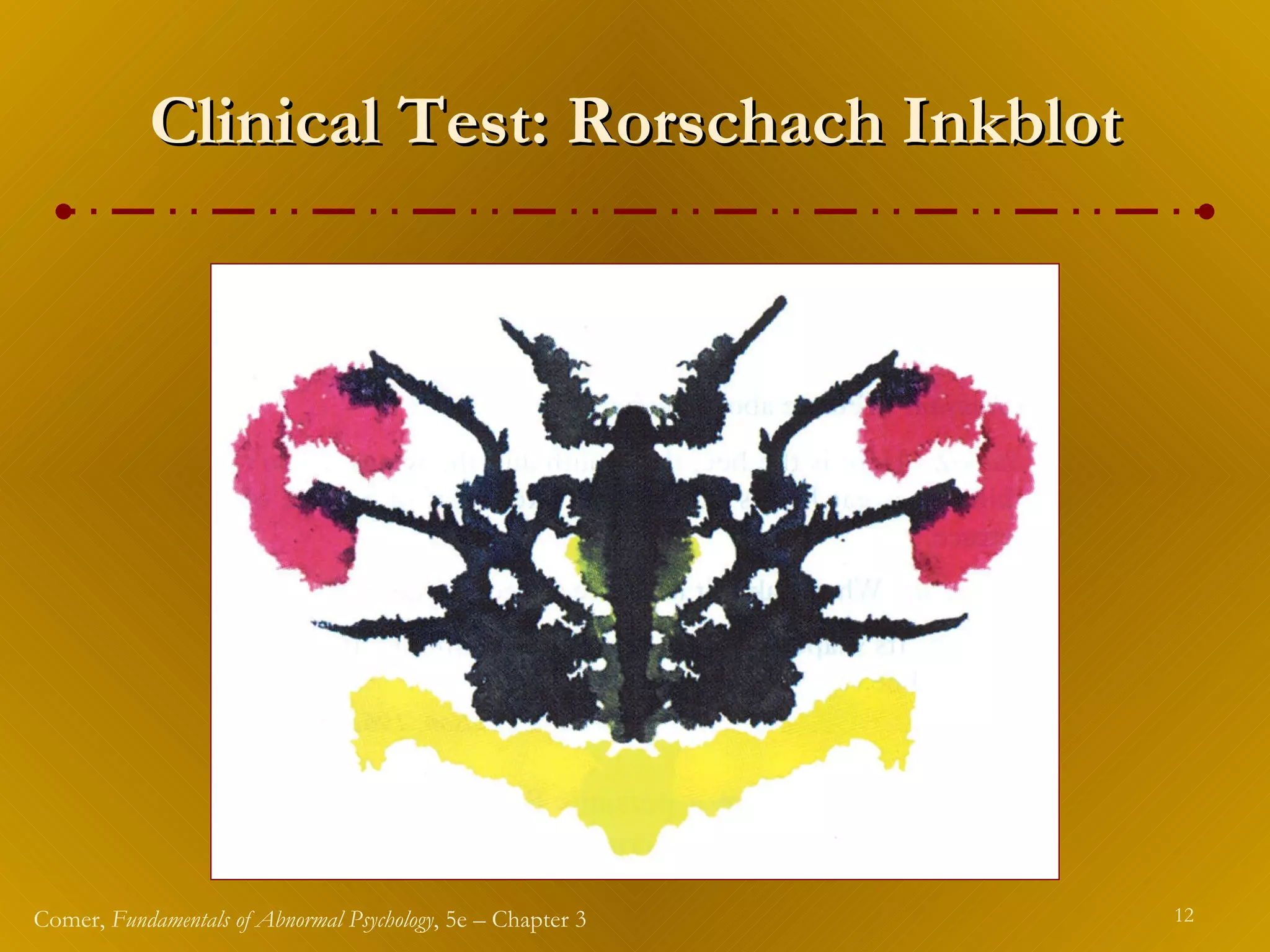
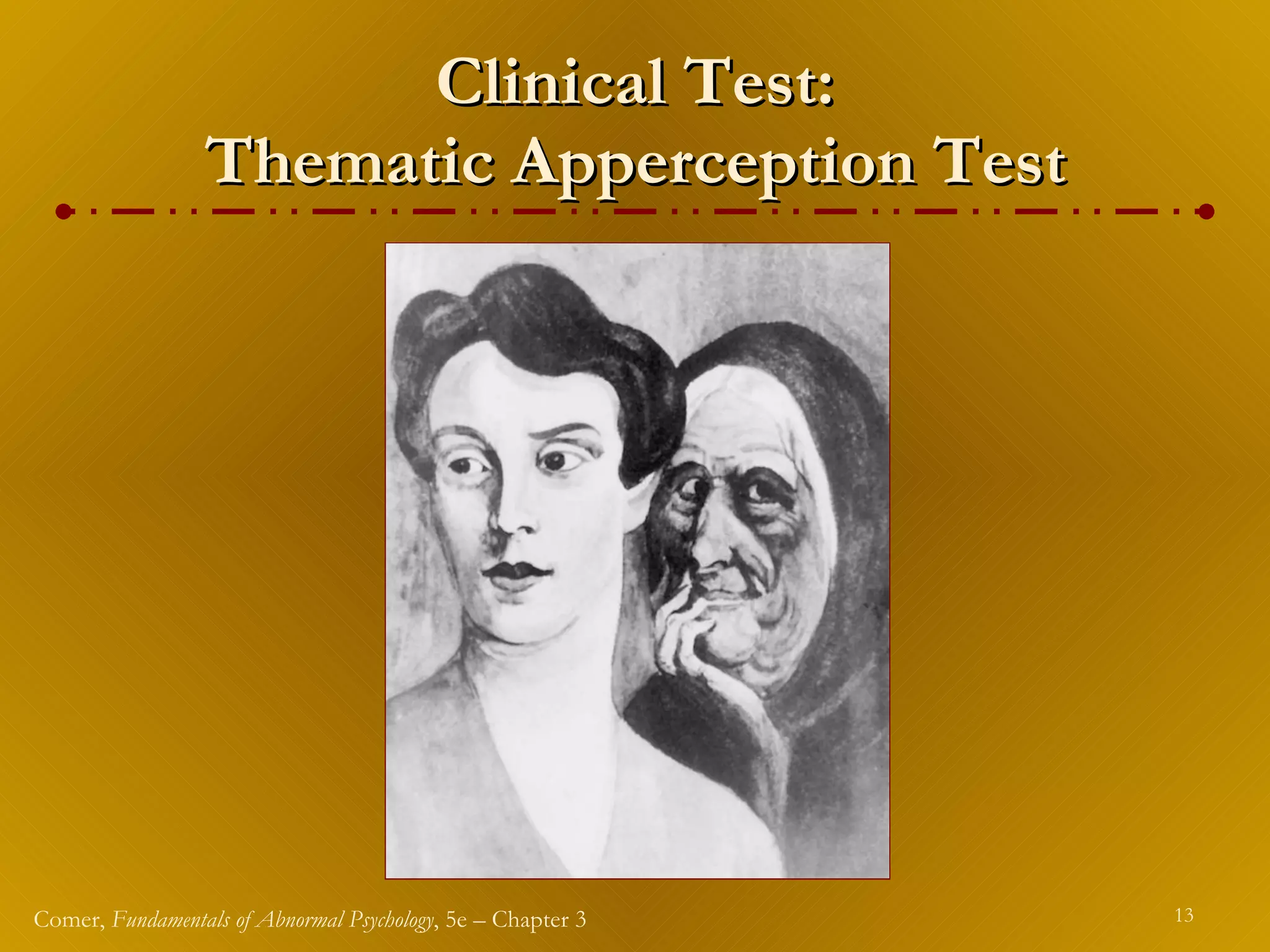
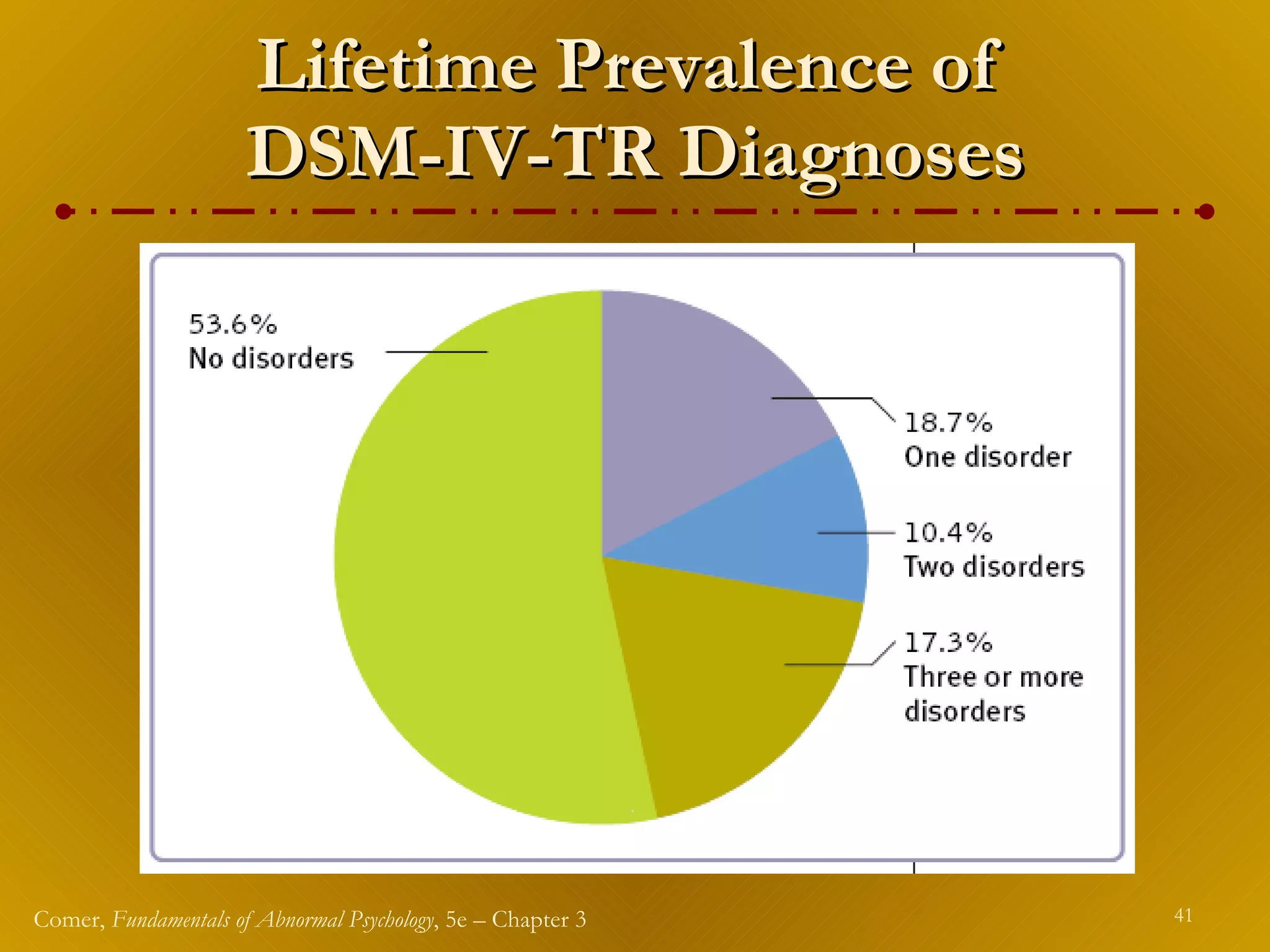
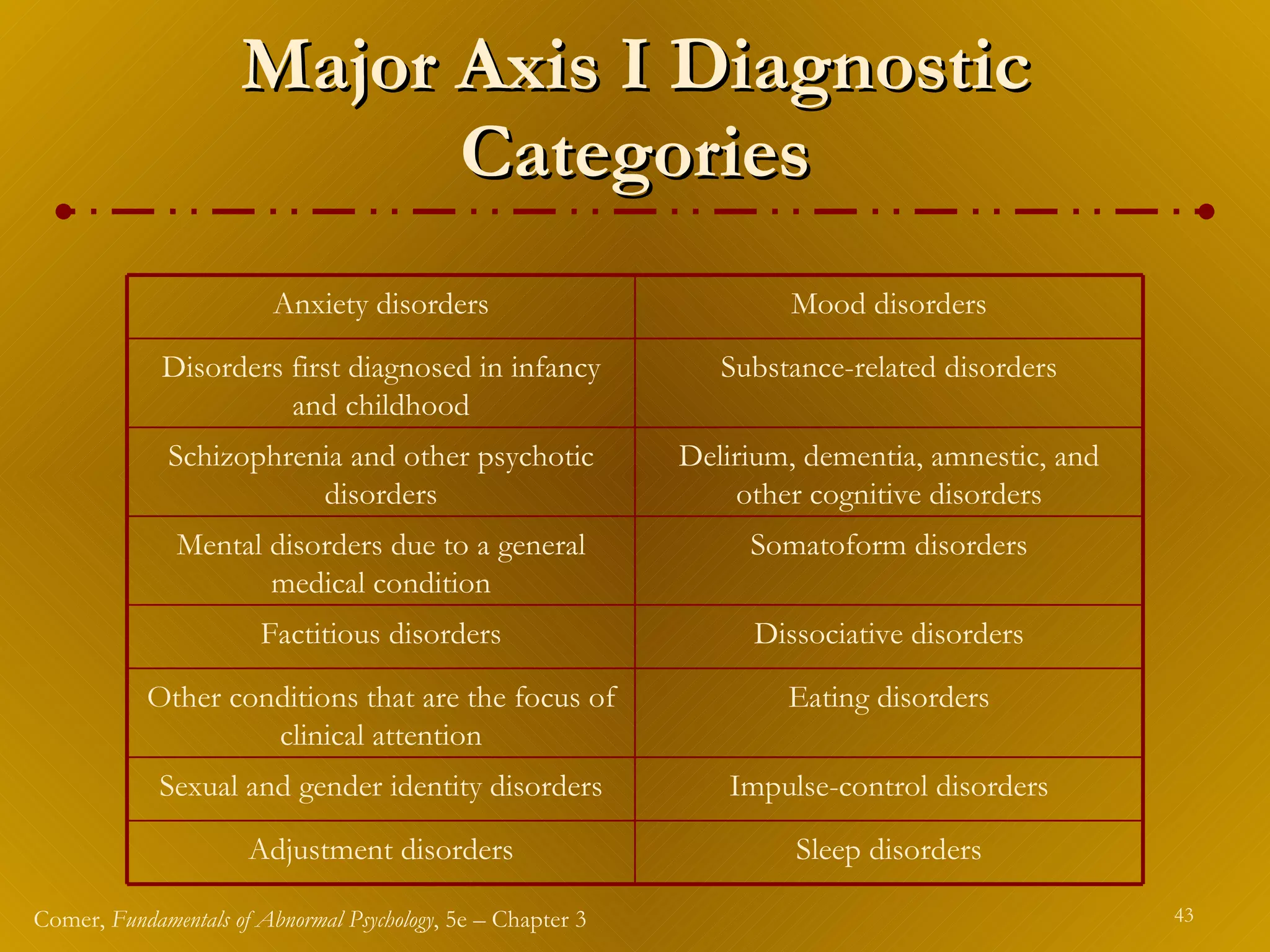
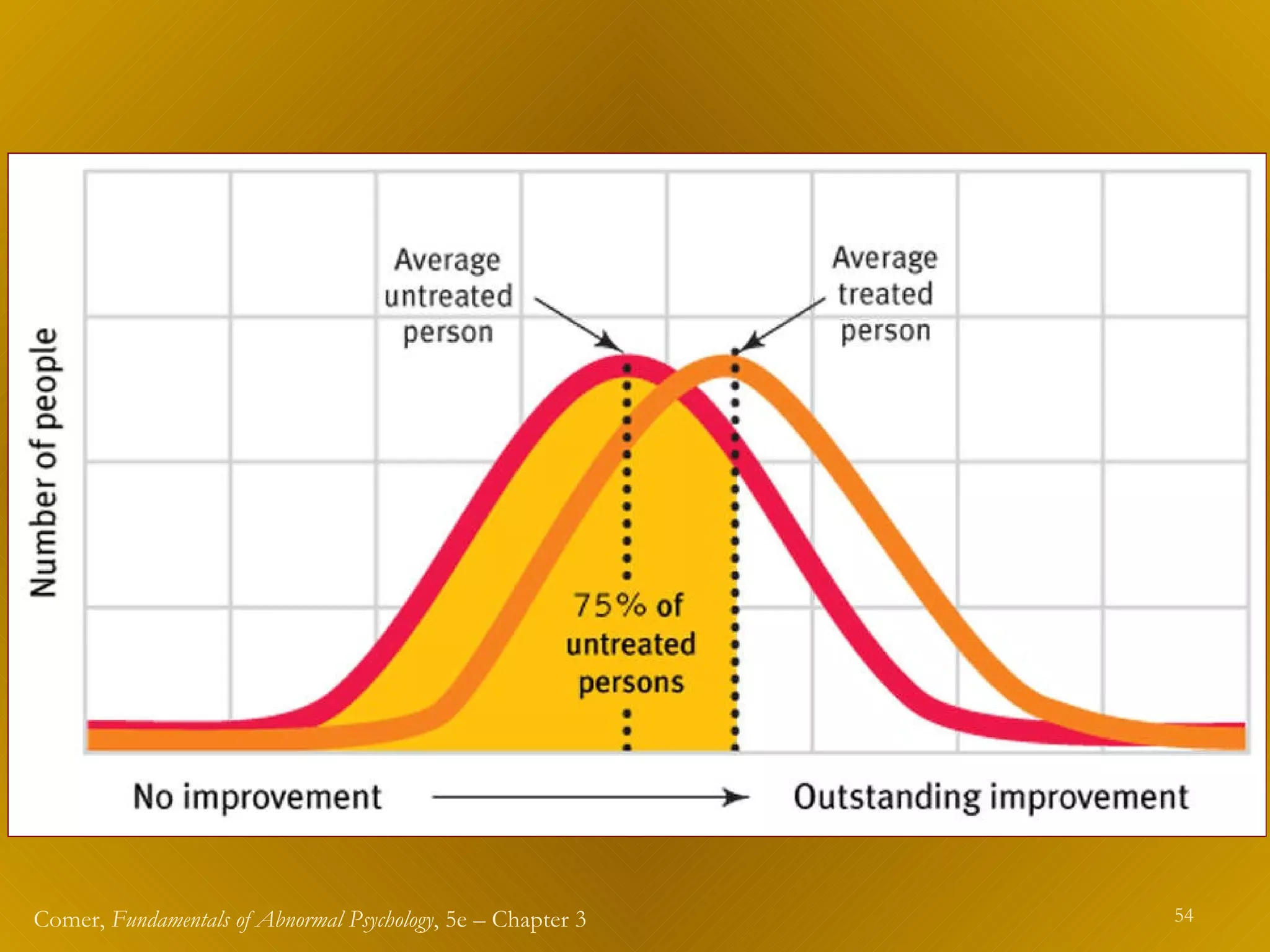
Clinical assessment involves collecting information to determine how and why a person is behaving abnormally and how they can be helped. Clinicians use clinical interviews, tests, and observations as assessment tools, which must be standardized, reliable, and valid. The DSM-IV-TR is commonly used for diagnosis and describes diagnostic criteria across five axes. Treatment decisions are based on assessment and diagnosis information, with the goal of empirically supported and evidence-based therapies. Research shows that therapy is generally more effective than no treatment, though some therapies may be more effective than others for specific problems.



![Psychodiagnostic technique[1]](https://cdn.slidesharecdn.com/ss_thumbnails/psychodiagnostictechnique1-191031121907-thumbnail.jpg?width=640&height=640&fit=bounds)