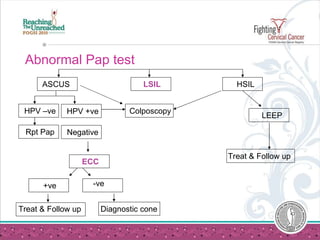
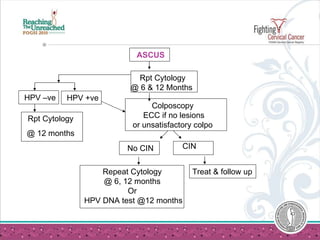
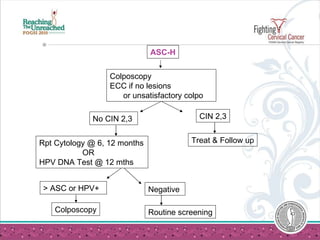
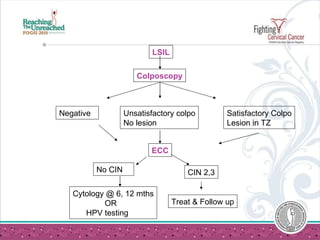
The document provides guidelines for managing abnormal Pap test results. It discusses recommendations for atypical squamous cells of undetermined significance (ASC-US), atypical squamous cells cannot exclude HSIL (ASC-H), low-grade squamous intraepithelial lesion (LSIL), and high-grade squamous intraepithelial lesion (HSIL). It recommends repeated testing, HPV testing, or colposcopy and possible excision depending on the abnormality and test results. It also covers atypical glandular cells, management of cervical intraepithelial neoplasia, and special considerations for adolescents, pregnant women, and postmenopausal women.










































































![Getting Started with Apache Spark: Big Data Made Simple [Free Meetup]](https://cdn.slidesharecdn.com/ss_thumbnails/apachesparkgettingstarted-260203175547-8361bcc3-thumbnail.jpg?width=640&height=640&fit=bounds)









