Downloaded 200 times


























![SLN Mapping
• As a trade-off between lymphadenectomy and no surgical assessment at all in
patients with endometrial cancer, there has been interest in adopting a sentinel
lymph node approach similar to that in breast cancer
• Results from these two studies ( MKSCC[226 patients] and French Trial[125
patients] ) suggest that SLN mapping is feasible and that adding SLN mapping
to surgical staging procedures seems to increase the likelihood of detecting
metastatic cancer cells in regional lymph nodes.
• Whether sentinel lymph node mapping will replace lymphadenectomy needs to
be determined](https://image.slidesharecdn.com/caendometrium-ii-170102181105/85/Ca-endometrium-29-320.jpg)



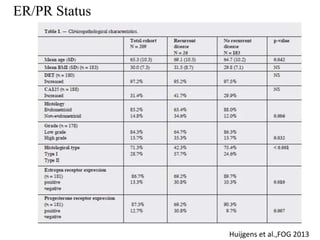






Endometrial cancer most commonly presents with postmenopausal vaginal bleeding. Histopathology shows endometrioid adenocarcinoma in 75-80% of cases. There are two types - type I is estrogen-dependent and has a better prognosis, while type II is more aggressive and has a poorer prognosis. Diagnosis involves endometrial biopsy or dilation and curettage. Staging involves surgical procedures like total abdominal hysterectomy and lymph node sampling or dissection. Prognosis depends on factors like age, grade, histology, lymph node involvement and stage.




















































































