Downloaded 417 times









![ Discontinuing screening :
— The age to discontinue screening in older women
depends on whether or not they have received adequate
prior screening.
Adequate prior screening — In general, we
suggest not screening women aged 65 years and older
provided they meet the following criteria:
No increased risk (ie, history of abnormal screening,
current smoker or history of smoking, unknown screening
history, previous HPV-related disease, new partners,
immunocompromised, in utero diethylstilbestrol
exposure)
Adequate prior screening: two negative consecutive co-
tests or three negative Pap tests within the past 10 years,
with the most recent test within the previous five years
[43]
No history of high-grade dysplasia or worse](https://image.slidesharecdn.com/cancercervixscreening-150610155239-lva1-app6892/85/Cancer-cervix-screening-11-320.jpg)
















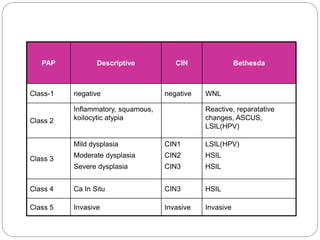



This document discusses cervical cancer screening. It begins with the epidemiology of cervical cancer, noting it is the 3rd most common gynecologic cancer in the US but 2nd most common in countries without screening. Risk factors include early sexual activity, multiple partners, HPV infection, and low socioeconomic status. Screening with Pap tests has reduced cervical cancer rates by 70% in the US. The document then discusses screening guidelines, techniques for Pap tests, interpreting results, HPV vaccination, and screening special populations like immunocompromised women.